
Remember me
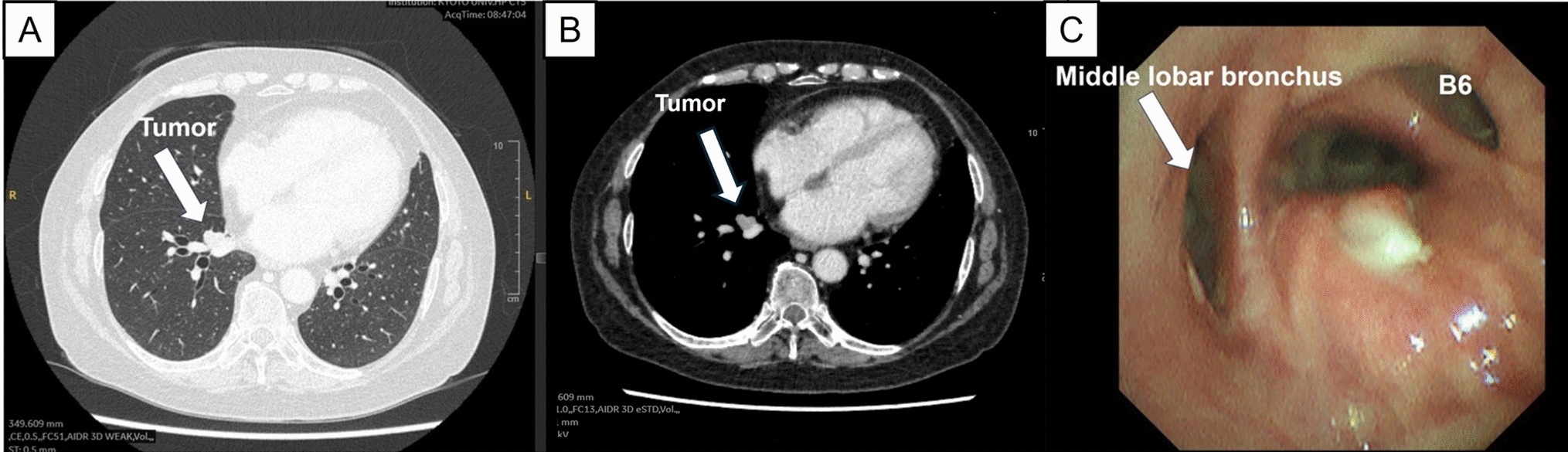





A 64-year-old female former smoker presented with a lung mass. She had a history of rheumatoid arthritis and had been receiving long-term steroid and biological treatment. Chest computed tomography (CT) revealed a 1.8-cm tumor occluding B7 and a 1.7-cm cavity with an irregularly thickened wall in segment 2 of the right upper lobe. Staging positron emission tomography/CT showed maximum standardized uptake values of 5.6 in the S7 tumor and 4.7 in the S2 tumor without evidence of regional lymphadenopathy (Fig. 1A, B). Bronchoscopy confirmed that B7 was completely occluded by a tumor that invaded the bronchus intermedius, resulting in a diagnosis of double squamous cell carcinoma (cT1bN0M0: S2 and S7; Fig. 1C). Preoperative respiratory function tests were as follows: vital capacity, 2810 mL (83.3%); forced expiratory volume in 1 s, 1900 mL (84.4%); and percent predicted diffusing capacity of the lung for carbon monoxide, 63.5%. Because chest CT suggested slight emphysematous and fibrotic changes and the patient had rheumatoid arthritis, we were concerned about the possibility of interstitial pneumonia. Therefore, we recommend surgical resection rather than radiotherapy. Given the proximity of the tumor to the orifices of the middle lobar bronchus and B6, we planned sleeve basal segmentectomy combined with S2 wedge resection to preserve the middle lobe and S6.
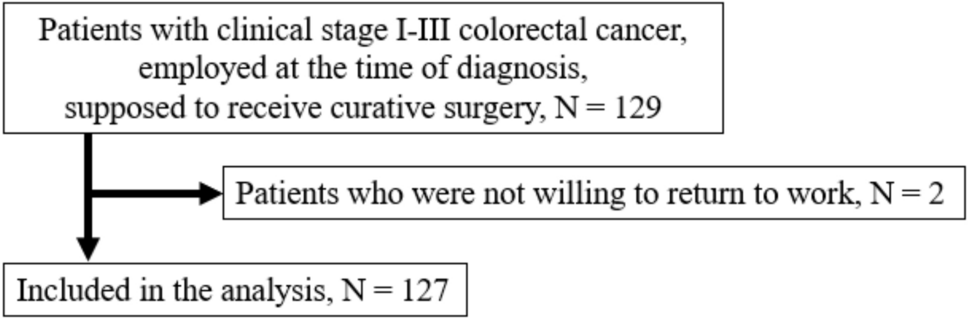
Fig. 1
Preoperative findings. A, B Chest computed tomography showed a 1.8-cm tumor in S7. C Bronchoscopy revealed complete occlusion of B7 by the tumor, which had invaded the bronchus intermedius
Surgical techniques and operative findingsAfter obtaining written informed consent from the patient, the S2 cavitary lesion was first removed through posterolateral thoracotomy in the fifth intercostal space. The tumor was palpable as an elastic soft mass. To minimize pulmonary resection, electrocautery was used to outline the planned resection line on the pleural surface; the line accounted for the tumor plus a 10-mm surgical margin. The pulmonary parenchyma was gradually divided, and the deepest portion of the tumor was resected using a linear stapler. Next, we performed basal sleeve segmentectomy. After exposing the interlobar pulmonary artery, the basal artery was divided and closed with a running 6–0 polypropylene suture, while the interlobar artery was controlled proximally using a vascular clamp. The indocyanine green technique was then used to demarcate the segmental line, facilitating division of the S6 and basal segments with a stapler. The hilar lymph nodes (#7, 10, 11s, and 12l) were dissected. The proximal and distal transection lines at the bronchus were carefully determined, and the middle lobar bronchus, B6, and bronchus intermedius were transected using a sharp scalpel, maintaining at least a 1-cm gross surgical margin (Fig. 2).
Fig. 2
Intraoperative findings before cutting the basal bronchus. The basal bronchus was carefully transected using a sharp scalpel while maintaining a gross surgical margin of at least 1 cm
After confirmation of a negative central bronchial margin using a frozen section, bronchial reconstruction with double-barrel anastomosis using B6 and the middle lobar bronchus was attempted. However, the anastomosis site was completely obstructed behind the A6. To ensure an adequate surgical view for bronchial suturing, A6 was divided after proximal clamping of the interlobar artery and distal clamping of V6 under systemic heparinization (2000 U bolus) (Fig. 3A, B). The deepest area, including the middle lobar bronchus and the bronchus intermedius, was anastomosed using a running 5–0 polydioxanone suture. Subsequently, B6 and the bronchus intermedius were anastomosed. A few adjusting tack sutures were placed in the membranous part of the bronchus intermedius to minimize caliber difference, allowing for successful completion of the double-barrel anastomosis using a running suture. All of the knots were tied externally (Fig. 3C, D). Once the double-barrel anastomosis was completed, A6 was reconstructed using a running 6–0 polypropylene suture. Reventilation resulted in prompt lung expansion. Finally, the bronchial anastomosis was covered with a pedicle fat pad. The total operative time was 318 min. The estimated blood loss volume was 170 mL.
Fig. 3
Intraoperative findings after bronchial resection. A, B A6 was divided after sleeve basal segmentectomy was performed. C, D Sufficient surgical exposure was achieved after division
Postoperative courseThe patient’s postoperative course was uneventful. After confirming adequate bronchial healing via bronchoscopy and CT on postoperative day 7, the chest drain was removed. The patient was discharged 3 days later. A postoperative histopathological examination revealed double squamous cell lung cancer with 12-mm surgical margins (S2:13 mm, pT1bN0; S7:28 mm, pT1cN0). At the 6-month follow-up, bronchoscopy showed excellent healing of the anastomosis without recurrence, and contrast-enhanced CT showed sufficient A6 blood flow (Fig. 4A, B, video).
Fig. 4
Postoperative findings. A Bronchoscopy performed 6 months after the surgery revealed excellent bronchial healing. B Contrast-enhanced computed tomography indicated sufficient A6 blood flow
Comments (0)