
Remember me


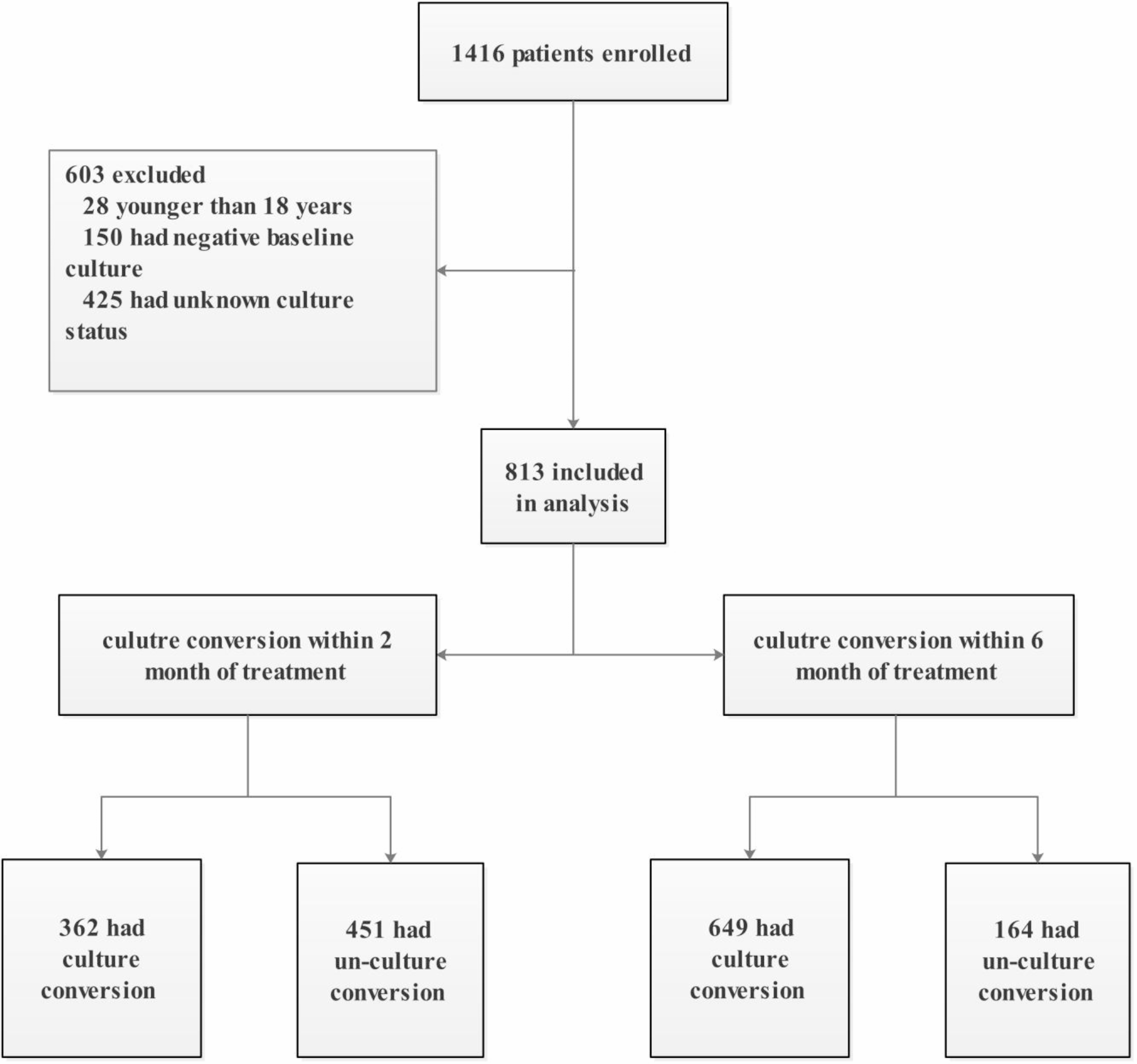
The workflow and time required for specific tasks or during specific time periods varied from case to case (Fig. 1). Workflow in DOSA involved 6–7 staff who sequentially did specific tasks. Workflow in the operating room while patients were conscious involved 8–9 staff who performed multiple tasks simultaneously. The sequential workflow was the main advantage of applying PVI in DOSA. However, if a case is delayed, the time from application to incision could be longer than optimal.
Fig. 1
Timeline from the time patients entered DOSA until their incisions were made (n = 3). The blue stars represent possible points in the process when patients are conscious and PVI could be administered.
The time proximity to the incision and the circulating nurses’ interactions with conscious patients were advantages to applying PVI in the operating room; however, the complex workflow in the operating room could increase the likelihood that PVI would not be given. The task and timeline analyses suggested that either the DOSA nurse or the circulating nurse would be best situated to apply PVI depending on whether PVI is applied in DOSA or the operating room. In DOSA, the patient is conscious and there is more downtime. Given that the manufacturer recommends administering PVI within one hour before surgery, we chose to apply PVI near the end of the patient’s time in DOSA.
Semi-structured interviewsWe conducted semi-structured qualitative interviews with four healthcare workers. Two DOSA nurses, one postoperative nurse, and one orthopedic trauma surgeon agreed to be interviewed.
Visual aids facilitated PVI administrationTwo of the nurses indicated that visual aids facilitated PVI administration. A poster listing step-by-step instructions for PVI administration was available inside a medication room and this poster served as a “refresher” for a nurse who administrated PVI infrequently during the study. She stated, “…I don’t need like a rundown like every little tiny detail, I need like how many times do I do it and for how long, you know? I feel like that poster was very like succinct and short and it was like okay, I got it” (Postoperative Nurse). This nurse found the visual poster more useful than the text-based educational materials our researchers provided to staff at the beginning of the intervention. Another staff nurse participant suggested that a sign in the patient’s room describing the purpose of nasal PVI or a patient information pamphlet would encourage patients to accept the intranasal PVI.
Low staff and patient burden facilitated PVI implementation into existing workflowAll three nurses agreed that while integrating PVI into their existing workflow added a few minutes of work, they believed staff would eventually adopt the intervention because the time required to apply the PVI is minimal, the swab is noninvasive, and intranasal PVI could prevent infections. Nurses already administer several pre-operative infection prevention precautions to patients, including chlorhexidine bathing for all surgical patients and routine MRSA and COVID nasal screening. Staff were willing to integrate PVI into their infection prevention practices due to its role in infection prevention. A DOSA nurse noted, “It just seems like part of the process you know; this is what we do to get you ready.”
Having patients self-administer PVI would facilitate staff workflowPatients sometimes confused the PVI and COVID swabs, and staff offered solutions for increasing the likelihood that patients would find having PVI applied to their nares acceptable. For example, one nurse noted that patients were more receptive to the PVI swab after she explained that the swab would not extend beyond the inside of the nares. A different staff nurse suggested that having patients self-administer the PVI swab would ease workflow and give patients more control over the process: “…instead of talking about why it would be uncomfortable, if [patients] just kind of did it themselves… I think it would be quicker accepted and easier for the patients” (DOSA Nurse).
Emphasizing PVI efficacy to staff and patients incentivized adoptionWhen asked what could make the intervention more successful, all four interviewees stated that showing staff and patients evidence that use of PVI prevents SSI infection would facilitate PVI adoption. A DOSA nurse noted,
You know does it take a few more minutes? Yes. Um…but is it worth it? Probably. You know if the research shows that it’s worth it and it helps prevent infection then it’s worth doing.
The orthopedic surgeon also suggested that educating staff about the evidence for PVI’s efficacy would facilitate implementation in this hospital and in others. Similarly, the four participants indicated that educating patients about PVI’s efficacy would encourage patients to accept this intervention. A DOSA nurse remarked that, “I love the research part of it. So if a patient asked us questions we could look professional in answering that question, this is why we’re using it, we appreciate you participating in it and these are the outcomes that we are experiencing and explain to them in terms that they can understand the effectiveness…”.
Including nasal PVI with medications in EMR facilitated implementation for some staff rolesThe nurse participants felt that having PVI orders with other medication orders in the electronic medical record (EMR) was a key facilitator because it helped them identify the patients who were enrolled in the study and required PVI. A DOSA nurse described the process this way: “If the swabs were ordered pre-op, they would already be in the order set so that we knew that the patient was… a patient that was going to be in the study and we need to do the swabs so it kind of gave us the heads up that the patient would have that.” In contrast, the orthopedic trauma surgeon—who was tasked with entering PVI orders for each patient—found that it increased his workload because placing the order took 2 to 5 min per patient. The surgeon suggested that PVI be included as a standing order for these patients to reduce this implementation barrier.
Barrier and facilitator concordance with the Expert Recommendations for Implementing Change (ERIC) FrameworkSeveral of the barriers and facilitators emerging from our analysis were concordant with implementation strategies identified in Powell’s Expert Recommendations for Implementing Change (ERIC) framework [13]. Concordant implementation strategies included conducting educational outreach visits; distributing educational material; involving patients/consumers and family members in the intervention; reminding clinicians; and promoting adaptability. We list these corresponding strategies in Table 1 with examples from our orthopedic trauma surgery context.
Table 1 Powell and colleagues’ Expert Recommendations for Implementing Change (ERIC) framework strategies concordant with those emerging from PVI administration in the studied orthopedic trauma surgery setting
Comments (0)