Baseline IPC and laboratory capacity assessment findings
The hospital IPC team consisted of four nurses, including one acting team leader. The hospital has an IPCC, but it had not been meeting regularly at the time of the baseline assessment. The microbiology laboratory had 10 laboratory scientists and technicians.
A three-hour facilitated tabletop exercise conducted on 11 May 2022 was attended by 34 participants. The ward walkthrough was conducted over two days (10 and 12 May 2022). A total of eight wards including acute medical and surgical wards, emergency, post-natal and ICUs were included in the walk-through assessment. Except for nurse unit managers (NUM), ward nurses worked 12-h shifts. The nurse-to-patient ratio ranged from 1:2 in the ICU to 1:5 in the acute and post-natal wards. The wards were multi-bed open layout with curtains between beds. Beds in several wards were spaced less than a metre apart. There were no single rooms with ensuite bathroom and toilet which could be used for isolation of patients with CRO infection or colonization. There was one isolation room (containing four beds) with a dedicated bathroom/ toilet in each acute ward. Visitors and family members often supported patient care on medical and surgical wards.
The main adult ICU had eight beds, two in each cubicle separated by a wall. Beds were well spaced apart. There were two separate isolation rooms adjacent to the main ICU which were not in use during the visit. The neonatal ICU (NICU) consisted of three separate rooms (all multi-bed) with a total of 24 bed capacity. One of the rooms (four beds) was used as an isolation ward. In addition, there was a stepdown room for NICU in the post-natal ward. The paediatric ICU was a single room with six beds. It had a separate isolation room (four bed) with a toilet. Shared handwashing sinks for patients (ranging from 1 to 3) were available in all wards. The adult ICU had one sink per bed. Most sinks were functional and equipped with soap and paper towels with HH education material displayed. Alcohol-based hand sanitizer bottles were usually available at the bed side or at a minimum at the entrance to a room. All patient toilet facilities on wards were shared (designated by gender), and most toilets did not have soap or paper towels available at the time of visit. Nurses interviewed stated that PPE was readily available for them.
Cleaning of the hospital was outsourced to a private company and the hygiene staff were shared between wards. Generally, the hygiene staff were responsible for all environmental cleaning except in high-risk wards such as ICU and the operating theatre where cleaning was done by ward assistants and nurses. A 3-step cleaning procedure (detergent and water, disinfectant and a final rinse with water) was used for environmental cleaning. Floor, surfaces and toilets were cleaned 2–3 times a day. Nurses were responsible for cleaning shared patient equipment at the bedside (e.g., stethoscope, blood pressure cuff), and for cleaning the immediate patient space (e.g., over bed table). Detergent/disinfectant wipes were not readily available on wards.
There were no locally adapted IPC SOPs available however, the 2010 general IPC guidelines developed by the Pacific Public Health Surveillance Network were referred to. There were also no specific SOPs for CRO case and contact management or environmental cleaning, although some flowcharts outlining cleaning procedures were sighted on the wards. There was no specific outbreak management plan for CRO outbreaks. However, staff reported that in 2017 a team from the WHO investigated a carbapenem resistant A. baumannii outbreak in NICU and recommended control measures. For risk communication, the treating medical and IPC teams usually informed patients and carers verbally about the CRO. There were no patient education leaflets or pamphlets regarding CRO.
The microbiology laboratory had the capacity to identify meropenem resistance using the disc-diffusion method and carbapenemase production using the modified carbapenemase inactivation method. There was no capacity to detect carbapenemase genes using polymerase chain reaction (PCR) or whole genome sequencing (WGS). There were approved SOP for all procedures performed in the laboratory.
Development and implementation of SOPs for IPC
A specific SOP for management of cases with CRO and their contacts was developed by the project team in consultation with the IPC team, wider hospital team and other local stakeholders. This was formally approved by the hospital IPCC in November 2022 and implemented through an education and training program. The recommendations within the SOP were informed by international publications [18,19,20], but were adapted for the local CWMH context. The main aim of the SOP was to provide evidence-based recommendations for prompt case detection and effective IPC management for priority pathogens including carbapenem resistant A. baumannii, E. coli, K. pneumoniae, and P. aeruginosa.
The preferred management of cases with CRO infection or colonisation is usually to isolate patients in a single room with its own ensuite with contact precautions (CP) in addition to standard precautions [18, 20]. However, at CWMH this was not practical to recommend. Therefore, it was agreed to isolate patients in a designated area within the wards further away from other patients and ensuring at least one metre between beds for IPC measures and patient/staff movement. An alternative isolation and CP strategy was cohorting patients with the same organism in the same four-bed isolation room. When CP were utilized at the bedside, a CP sign was placed close to the patient, a donning station was set up outside the patient zone and the doffing station inside the patient zone. Other recommendations included limiting movement of the patient, ensuring CP during any patient transfers, dedicating medical equipment where possible (or otherwise cleaning and disinfecting shared equipment after patient use), and daily cleaning of the patient zone. The procedure also advised on enhanced case finding using screening of high-risk groups and ward contacts (Supplementary Table S2). The SOP had a section on outbreak investigation and management.
Specific systems for notification and alert of patients infected or colonized with CRO were established. Pathways to ensure timely notification from the laboratory to ward staff, treating clinicians, IPC staff and hospital leadership were clarified with roles and responsibilities defined. The IPC team documented CRO notification on the front page of the patient’s medical folder and a CRO alert was added to the electronic patient information system for prompt identification of known CRO cases during subsequent admissions. Patients were provided with a CRO patient information leaflet and ward staff were educated on what information needed to be explained to patients and their care providers. IPC nurses also reviewed all CRO patients to ensure required IPC measures were in place.
Audit tools were developed to monitor compliance of HCW with recommended practices including appropriate patient placement/isolation, donning and doffing procedures and cleaning. Audit findings showed steady improvement in general donning and doffing practices. For example, the proportion of HCW who donned PPE in the correct order improved from 64% in 2023 to 76% in 2024. Similarly, 86% of HCW audited in 2024 followed the correct steps to remove PPE compared to 71% in 2023. HH compliance rates improved from 55 to 68% before donning and 31% to 48% after removing gloves.
Active screening for CRO colonization
Active screening on high-risk wards commenced in January 2023 which enabled early detection of CRO colonisation and appropriate management. Pre-emptive screening was conducted on all new adult ICU admissions and post-contact screening of patients who were deemed to be close contacts of any new case. For NICU, all newborns in the same room as a new case were deemed to be close contacts and were therefore screened. In addition, mother-newborn pairs were considered as close contacts and screened if either the mother’s or baby’s clinical or screening samples grew CRO. New admissions to the adult ICU were screened within 72 h of admission. Initially, post-contact screening was conducted seven days after detection of a new case. Due to a lack of a functional bed management system, it was not possible to follow up patients for this period of time. Therefore, post-contact screening was initiated immediately after confirmation of a case and a second sample was taken five to seven days later or before discharge when possible. Screening was conducted by collecting a rectal swab or stool for culture. Patient or guardian consent was obtained prior to collecting samples. The rate of ICU admission screening increased from 23% in January to 77% in December 2023. Overall, 70% of all new adult ICU admissions were screened in 2023. ICU admission screening continued through 2024, and coverage ranged from 31 to 71% in the first six months.
Development and implementation of laboratory SOP
New laboratory SOPs were developed to guide detection of CRO. This included SOPs for processing screening samples using CHROMAgarTM mSuperCARBATM, detection of carbapenem resistant genes using Xpert® CarbaR, storage of bacterial isolates in ultra-low temperature and preparation and shipment of isolates for WGS. All SOPs were approved for use by the Head of Pathology. Bench workflows were prepared for the new SOP. Other existing SOPs were revised and updated as needed. Essential consumables including meropenem discs and CRO selective media were procured. In addition, PCR testing kits for detection of five carbapenem resistance determining genes namely: blaKPC (KPC), blaNDM (NDM), blaVIM (VIM), blaOXA-48 (OXA-48), and blaIMP (IMP) were made available.
Development of environmental cleaning SOP
Following the baseline assessment of the IPC SOPs, it was determined that development of a general environmental cleaning SOP was a priority. A complete review of the cleaning practices, duties lists, products used, and audit tools was undertaken. A new 2-in-1 cleaning and disinfection product was introduced with the aim of simplifying environmental cleaning and disinfection in high priority wards (ICU, NICU and some acute wards). Roles and responsibilities for cleaning tasks were clarified and documented, as were daily and discharge cleaning checklists for patients with a CRO. Use of a fluorescent ultraviolet marker was included as part of the audit tools developed to assess compliance with the new procedures and for training proposes. The new SOP and audit tools were endorsed by the IPCC in June 2023. Two training sessions were conducted for 51 hygiene staff and nurses in March and May 2024. Audits (visual and fluorescent marker) conducted between January through July 2024 showed overall improvements in cleaning compliance.
Training of IPC and laboratory staff
The project team trained (onsite and online) the IPC team on the new CRO management SOP as well as monitoring and follow up strategies. Subsequently, the CWMH IPC team conducted regular training and education sessions for hospital staff. Refresher training for all IPC and CG teams was conducted before the end of the project. As part of a concurrent program (the COMBAT-AMR project funded by the Australian Department of Foreign Affairs and Trade) four laboratory staff were able to travel to Melbourne, Australia to receive in-depth training in August and September 2022. During project implementation, a series of structured training and AMR education sessions were organised [17]. After the project, the hospital team continued to train new staff and organised IPC workshops and awareness programs. The regular online mentorship and meetings with microbiologists and IPC specialists have continued beyond the project end date.
CRO communication and surveillance
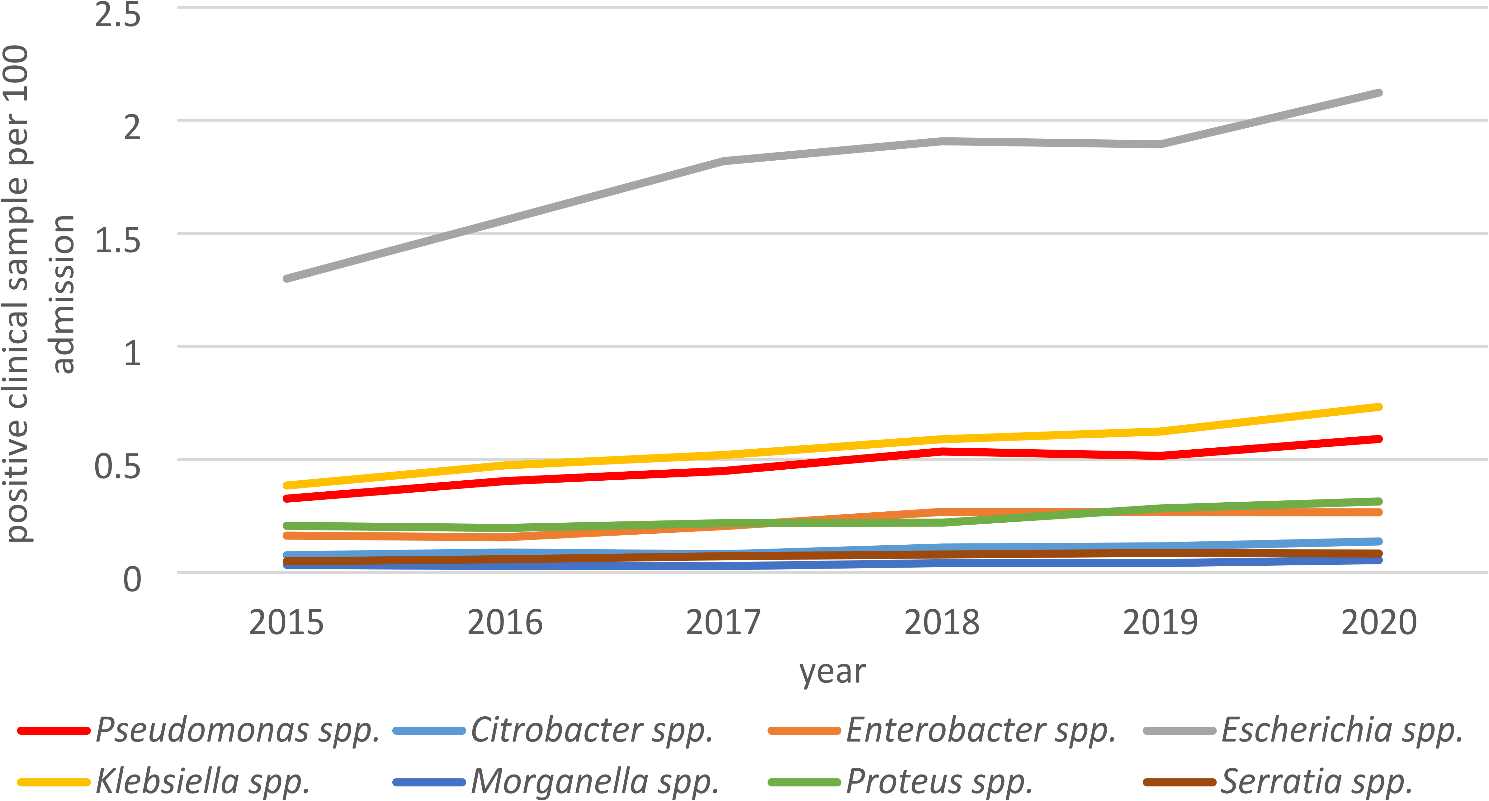
In addition to phone notification from the laboratory to the ward staff and IPC team, the laboratory team created a messaging group. Prompt reporting of laboratory results including type of CRO, the antimicrobial susceptibility pattern and carbapenemase production by phone and a messaging group enabled the IPC team to implement preventative measures immediately. The laboratory team established an online dashboard for CROs which is updated weekly and accessed by consultants to monitor case load. The IPC team also commenced collating CRO data which was shared with CG and consultants for effective case identification and management. The project also enabled a retrospective review of the microbiological data which provided a baseline antibiogram [14]. A. baumannii and P. aeruginosa were the most frequently reported CRO followed by E. coli and K. pneumoniae. Further genomic characterisation of isolates from infected and colonized patients identified NDM 1 & 7 and OXA-23 as predominant carbapenemases [15]. Other globally prevalent carbapenemase genes such as KPC and OXA-48 were uncommon in Fiji. These data were used to inform a revision of the empiric treatment guidelines for hospital acquired sepsis for patients in the ICU.
CRO outbreak control
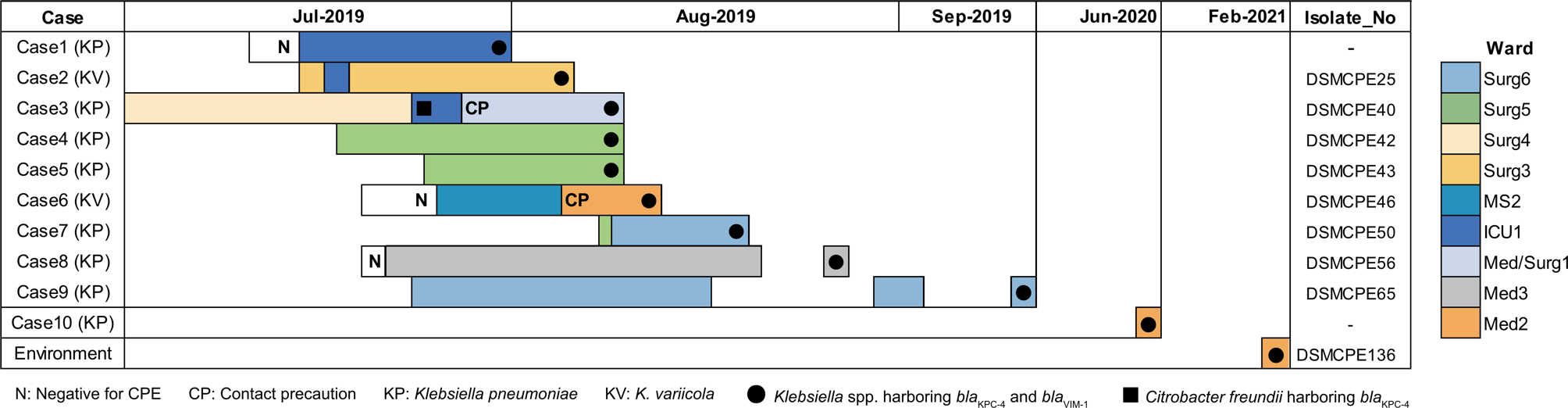
In January 2023, while this project was progressing, the ICU clinicians recognized a cluster of patients with CRO. The project team supported the local staff to use their SOP to identify, understand and manage the outbreak. A small taskforce of epidemiologists, IPC and ID physicians visited to rapidly assist local teams to examine the data that had been collected. Genomics were used to track likely transmission pathways. The team became aware that several concurrent CRO outbreaks in the ICU and acute wards were occurring [15]. An Outbreak Management Team (OMT) was established in May 2023 to coordinate the CRO outbreak responses in the hospital. The OMT membership is comprised of the medical superintendent, IPC team, NUMs of the affected wards, physicians, microbiology laboratory scientist, and environmental cleaning support services. The OMT oversee implementation of the hospital’s outbreak management plan, and all decisions and actions required for the outbreak response. Two CRO outbreaks were declared in NICU in June and August 2023. The OMT facilitated timely notification and reporting of cases as well as determining what additional resources and personnel were required to contain the outbreaks. The OMT continues to meet regularly, and recommendations are submitted to the IPCC for overall coordination.
As part of the CRO outbreak response, the OMT made a one-off submission to the National Medicine Therapeutics Committee for the procurement of newer and more effective antimicrobials including ceftazidime-avibactam + aztreonam, tigecycline and cefiderocol. The antimicrobials were procured by the Fiji MoHMS. Protocols for laboratory testing and treatment were prepared and the antimicrobials are currently in use for the treatment of CRO infections. The sustainability of procuring them can be challenging as the antimicrobials are not in the Fiji’s essential medicine list due to high cost.
Coordination of CRO interventions
The hospital IPCC is delegated by hospital management (medical superintendent) to be responsible for coordination, monitoring and evaluating the IPC programme. The IPCC membership includes the director of nursing, hospital administrator, head of CG, head of medical unit, sister-in charge, theatre manager, representatives from stores, and pharmacy. Their scope is to set the minimum standards for the IPC program in CWMH with adapted evidence-based/best practice SOPs, development of IPC capacity, raising awareness of IPC, and developing and maintaining IPC links through link nurses, medical staff and the laboratory department. Following the COVID pandemic, there has been increased recognition of IPC and CG roles in preventing transmission of infections within the hospital. Their positions were further supported in partnership with the CWMH administrators who provided the IPC team with a newly designated office space, which was subsequently renovated and equipped to enable the team's ability to fulfil their IPC responsibilities effectively. The new Fiji National IPC guidelines were released in May 2022. In collaboration with the Pacific Community and the Australasian College for Infection Prevention and Control, the Foundations of IPC course was undertaken by all CWMH IPC officers in 2023. Further IPC strengthening was undertaken at a national level which saw a significant review in the IPC consumable list to include approved cleaning and HH products that are aligned to the new IPC guidelines. The key lessons learned during project implementation and further opportunities for sustainability are listed in Supplementary Table S3.



Comments (0)