Study design
We performed a nationwide prospective cohort study of all adults hospitalized with TBE at departments of infectious diseases in Denmark between 1st of January 2015 and 31st of December 2023.
Setting
In December 2023, the total population of Denmark numbered 5.9 million people. In Denmark, healthcare is tax-financed and provided to all residents free of charge. A unique ten-digit personal identification number is assigned to all Danish residents at birth or upon immigration and can be used for linkage of all healthcare information at an individual level.
Data sources
The Danish Study Group of Infections of the Brain (DASGIB) is a nationwide, population-based, prospective cohort study enrolling all patients ≥ 18 years with a CNS infection managed by departments of infectious diseases in Denmark since 2015 [15]. We used the DASGIB database to identify all adults hospitalized with TBE in the inclusion period. Additionally, a cohort of matched controls with HSV-1 encephalitis was identified. Subjects were matched 1:1 on sex and age ± 5 years. One HSV-1 patient was used as a control for two different TBE patients due to lacking matches.
TBE diagnostics (polymerase chain reaction (PCR) and serology) are centralized at SSI. TBEV-IgM and –IgG antibodies in serum and/or cerebrospinal fluid (CSF) were measured using the Serion FSME/TBE Virus ELISA (Serion Diagnostics, Germany) following instructions of the manufacturer. TBEV-RNA in serum and/or CSF was detected with real-time PCR.
To calculate the yearly incidence of TBE from 2015 to 2023, numbers on all second phase TBE cases, including sex and age (including patients < 18 years), were retrieved from SSI [13]. Numbers on the yearly Danish population including sex and age were retrieved from Statistics Denmark, the central authority on Danish statistics [16].
To calculate the yearly test rate of TBE from 2015 to 2023, data on TBE tests were retrieved from The Danish Microbiology Database (MiBa) (including patients < 18 years). MiBa is a nationwide, automatically updated database of all microbiological test results in Denmark [17]. Every tested person only appeared once, regardless of the number of tests, per calendar year from 2015 to 2023.
Study population
Study participants fulfilled the DASGIB criteria for CNS infections [15]. Meningitis was defined as a clinical presentation consistent with viral meningitis (e.g., headache, neck stiffness, photophobia, hyperacusis, fever) without signs of encephalitis. Encephalitis was defined according to the International Encephalitis consortium [18]. Meningoencephalomyelitis/-radiculitis was defined as encephalitis with involvement of the spinal cord or spinal nerve roots. Pleocytosis was defined as ≥ 10 × 106 cells/L in the CSF [15].
Patients with TBE were defined by either a) detection of TBEV-IgM and -IgG antibodies in serum, b) TBEV-IgM in CSF, c) seroconversion or four-fold increase of TBEV-specific antibodies in paired serum samples, or d) detection of TBEV RNA by PCR in blood or CSF [19, 20].
Patients with HSV-1 encephalitis had a clinical presentation consistent with encephalitis and at least one of the following: a) detection of HSV-1 DNA in CSF by PCR or b) positive HSV-1 intrathecal antibody index test [21].
VariablesTBE patients
We obtained data on date and place of admission, basic demographics (age, sex, physical and functional status before admission), travel history, vaccination status for TBE and other flaviviruses (dengue, yellow-fever, and Japanese encephalitis virus), Charlson Comorbidity Index (CCI) score [22], immunodeficiency, history of tick bite, geographic location for tick bite, duration of symptoms, defined time from onset of symptoms to admission to hospital, clinical presentation, length of hospital stay, admission to the intensive care unit (ICU), and diagnostic work-up (biochemical and microbiological analyses of blood and CSF, and neuroimaging). Data on vaccination status were retrieved from the Danish Vaccination Register [23]. Immunodeficiency was defined as receiving treatment with immune-suppressive chemotherapy or corticosteroids, solid or hematological cancer, alcohol abuse, diabetes mellitus, congenital or acquired immunodeficiency, including human immunodeficiency virus infection [15].
The clinical presentation of TBE was classified as mild, moderate, or severe in accordance with previously published classifications [24]. Mild disease was defined as symptoms consistent with viral meningitis. Moderate disease was defined as slightly altered consciousness and/or diffuse or focal neurological symptoms. Severe disease was defined as altered consciousness and/or multifocal neurological symptoms. All patients with signs of encephalitis were classified as having moderate or severe disease.
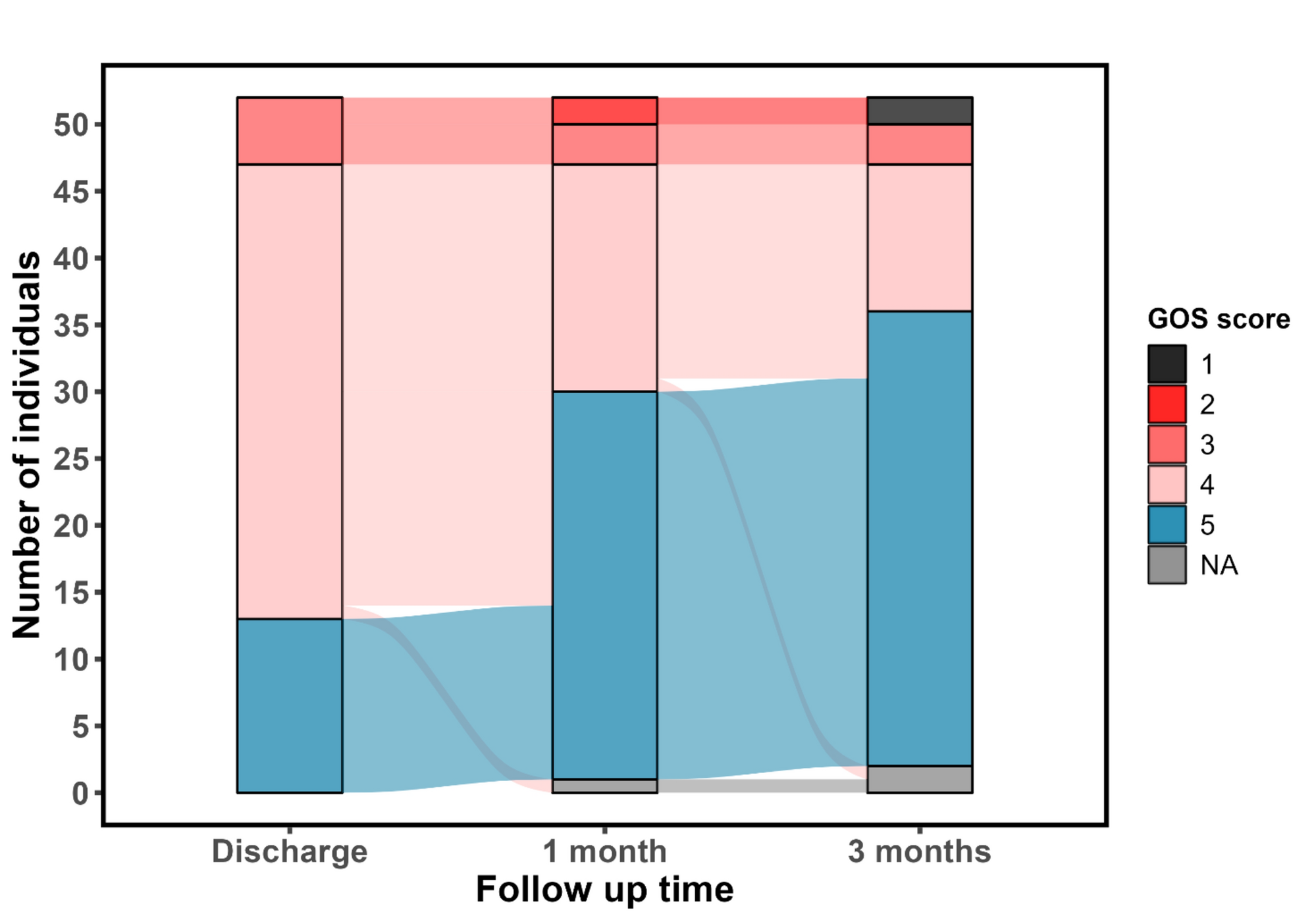
Outcome was measured as the Glasgow Outcome Scale (GOS) score: (1) Death, (2) A vegetative state, (3) Severe sequelae and dependency upon others in daily life, (4) Moderate sequelae but with the ability to live independently, and (5) No or only mild sequelae [25]. GOS score 1–4 was categorized as an unfavorable outcome. GOS score was registered at three timepoints: Discharge, 1-month, and 3-month follow-up. In case of a missing value, the GOS score at the previous timepoint was carried forward, if the patient had a favorable outcome (i.e., GOS score 5) or death (i.e., GOS score 1). Furthermore, information on self-reported residual symptoms in terms of fatigue, headache, cognitive impairment (memory and concentration), irritability, impaired hearing or hyperacusis, and objective residual symptoms such as speech disturbances, paresis, and paresthesia were retrieved at 6-month follow-up or later.
HSV-1 patients
We obtained data on date and place of admission, basic demographics, CCI score, immunodeficiency, admission to the ICU, diagnostic work-up in terms of neuroimaging, and GOS score at discharge, 1-month, and 3-month follow-up.
Statistical analysis
Categorical variables were reported as proportions and percentages, and continuous variables as medians, with interquartile ranges (IQR). The difference in age means was analyzed with an unpaired t-test. Differences in the likelihood of an unfavorable outcome (GOS score 1–4) between the TBE cohort and the HSV-1 cohort were evaluated at three timepoints (discharge, 1-month, and 3-month follow-up) using a logistic regression model accounting for age and sex. Analyses were repeated exclusively on the subgroup of TBE patients with encephalitis and their respective matched HSV-1 case. All analyses were performed using R (version 4.3.2) [26]. Logistic regressions were done with the glm function from the stats package [27]. Incidence rates, test rates, and positivity rates were calculated based on SSI records of all TBE cases in the study period. The incidence rates were adjusted for the age and sex distribution in the population.
Ethical considerations
The DASGIB database is approved by the Danish Board of Health (record numbers 3–3013-2579/1), and this study is approved by The Danish Data Protection Agency (record number R-23066339). Patient consent or an approval from the local Ethics Committee is not needed for this type of study in Denmark. All data are managed in compliance with relevant data protection and privacy regulations and in accordance with the Helsinki declaration.







Comments (0)