
Remember me



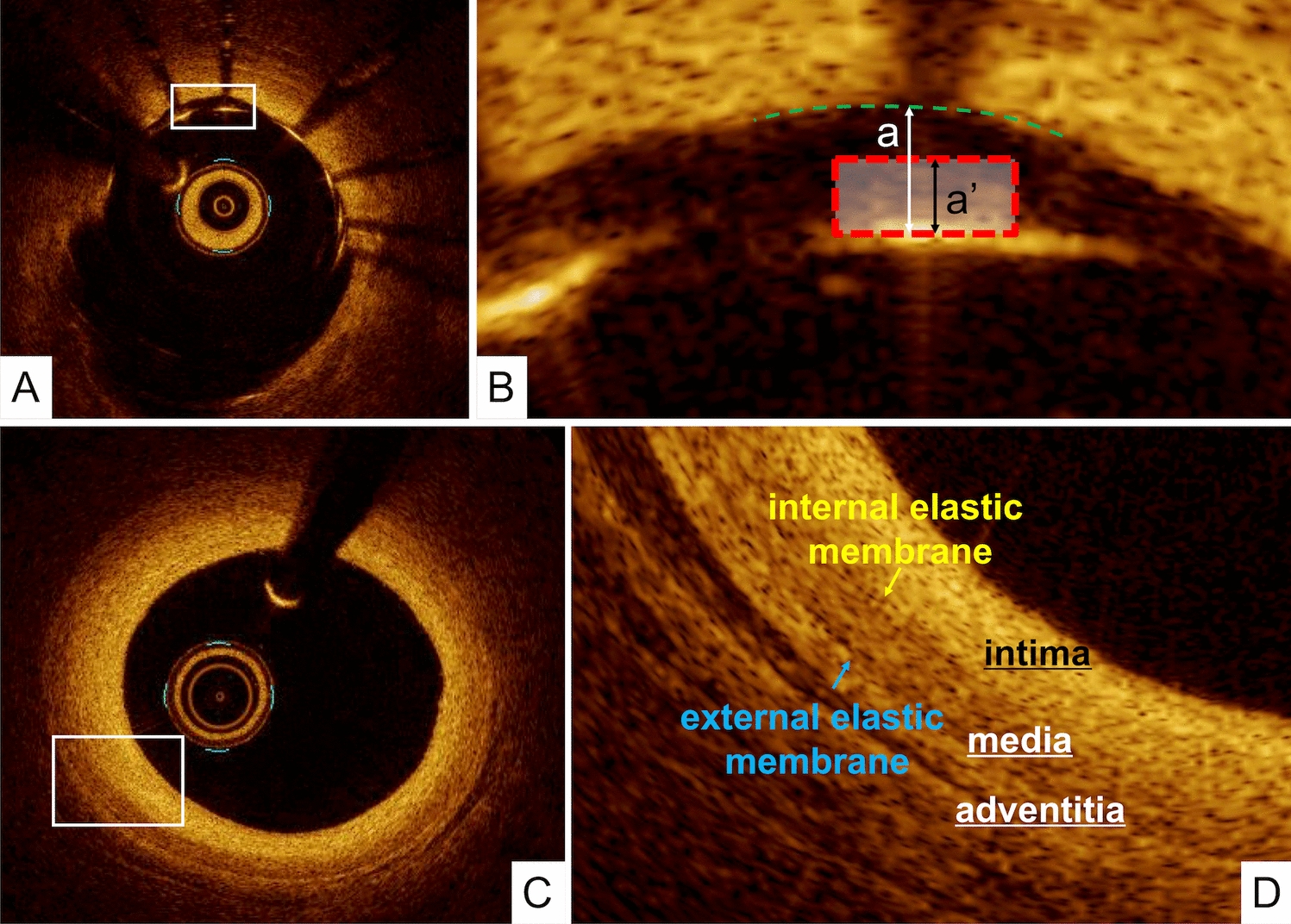


The normal coronary artery consists of three layers: the intima, consisting of the endothelium and collagen fibers; the media, consisting of smooth muscle cells and elastic fibers; and the adventitia, consisting of collagen fibers and surrounding fat. Because OCT measures the intensity of light returning from a tissue, tissues with a higher heterogeneity in the refractive optical index exhibit stronger optical scattering, and therefore, a stronger OCT signal. The intima in the normal arterial wall is usually represented by the high-intensity signal from the collagen fibers. The media appears as a homogeneous dark layer because of the presence of less collagen fibers and abundant smooth muscle cells and extracellular matrix. The adventitia is also represented by the high-intensity signal from the collagen fibers. (Fig. 1).
Plaque morphologyOCT is capable of differentiating lipid-rich plaque from fibrous plaque. Because OCT uses near-infrared light and cross-sectional images are generated by measuring the echo-time delay and intensity of light that is reflected or backscattered from the arterial wall, OCT can characterize tissue morphology by measuring the backscattered infrared light. In general, plaques can be characterized as fibrous, lipid-rich, or calcified, according to the plaque characterization criteria developed by histology-validation studies [9,10,11]. (Fig. 2).
Fig. 2
Fibrous, lipid-rich, and calcified plaques. A Fibrous plaque appears as a homogeneous high-intensity tissue with a gradual signal attenuation. B Lipid-rich plaque appears as low-signal-intensity regions with diffuse borders. C Calcified plaque appears as low-signal-intensity areas with sharply delineated borders
Fibrous plaques: These plaques consist of bundles of collagen fibers, smooth muscle cells, and extra-cellular matrix such as proteoglycan, and appear as a high-signal-intensity tissue because there is much reflected OCT light signal returning from the collagen fibers. Fibrous plaques represent the majority of atherosclerotic lesions. In general, the large amount of collagen fibers does not allow the visualization of the internal and external elastic membrane.
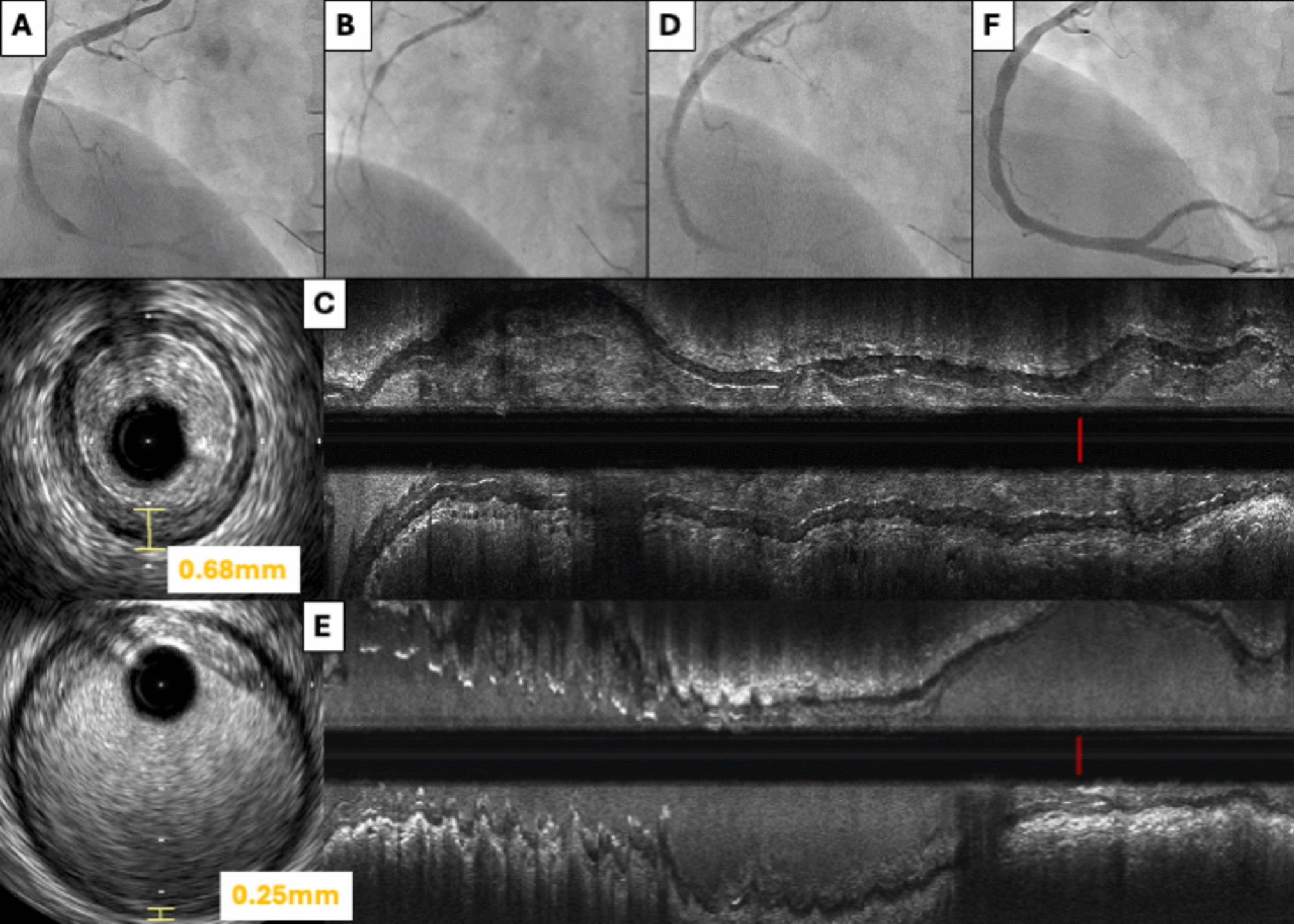
Lipid-rich plaques: These plaques appear as low-signal-intensity regions with diffuse borders because of considerable scattering of light of approximately 1000-nm wavelength from lipid components [12]. Fibroatheroma, which contains a necrotic core, cholesterol crystals, and foam cells, is considered as a representative tissue of a lipid-rich plaque. It should be noted that it is difficult to distinguish between the necrotic core and foam-cell accumulation on a single cross-sectional OCT image because these two tissues have similar OCT attenuation coefficients [13,14,15]. It has been postulated that thin-cap fibroatheroma (TCFA), which is characterized by a large necrotic core with an overlying thin fibrous cap, measuring < 65 µm, is the precursor plaque composition of plaque ruptures [16]. For OCT analysis, TCFA is usually defined as a plaque with lipid content with a fibrous cap measuring < 65 µm. (Fig. 3) The cap thickness should be measured at its thinnest region within the fibrous cap. However, it should be noted that imaging geometries with a small angle between the line of sight and the tangent to the lumen contour may lead to tangential signal dropout because the imaging beam cannot penetrate the vessel wall owing to strong scattering along an oblique line-of-sight. (Fig. 3C) Therefore, such sections should be interpreted with care.
Fig. 3
A representative image of thin-cap fibroatheroma. A OFDI image indicates signal-poor lesions with an overlying signal-rich band. B A magnified image of A. The minimum fibrous cap thickness was 50 µm. C A small angle between the line of sight (red line) and the tangent to the lumen contour (yellow line) could lead to a tangential signal dropout
Calcified plaques: These plaques appear as low-signal-intensity areas with sharply delineated borders. Because the dimensions of the individual particles of calcium hydroxyapatite are smaller than the wavelength of near-infrared light, there is little reflected light returning from these tissues. Thus, OCT images of dense calcium show weaker optical scattering and therefore, a lower OCT signal intensity.
In addition to fibrous, lipid-rich, and calcified plaques, the following morphology has been frequently found in patients with acute coronary syndrome on OCT.
Plaque rupture: A ruptured plaque is defined as a plaque with intimal tearing, disruption, or dissection of the cap. On injection of optically transparent crystalloid or radiocontrast media, these defects may have little or no OCT signal and may appear as cavities.
Erosion: OCT-derived erosion could be composed of intracoronary thrombus attaching to the luminal surface without detectable signs of fibrous cap rupture. However, it should be noted that the resolution of OCT may be insufficient for directly visualizing one layer of endothelial cells in the form of a 5-μm thick cellular monolayer, although OCT has a higher resolution than any other imaging modality,
Calcified nodule: A calcified nodule, which also has the potential to develop into coronary thrombosis, is defined as a high-backscattering mass protruding into the lumen with a strong signal attenuation and an irregular surface [17]. (Fig. 4) The calcified nodule often contains fibrin between the bony spicules, along with osteoblasts, osteoclasts, and inflammatory cells. It should be noted that the OCT image of a calcified nodule is similar to that of a red thrombus, although a calcified nodule usually coexists with a calcified sheet in the same segments.
Fig. 4
A representative image of a calcified nodule. A OFDI image showing a high-backscattering protruding mass with an irregular surface, following a low-intensity area with a diffuse border (arrowheads) such as a red thrombus. B A magnified image of A
The other plaque morphologies can be evaluated using OCT.
Thrombus: A thrombus appears as an intramural mobile mass attached to the luminal surface or floating within the lumen. OCT can be used to classify a thrombus as a red or white thrombus. A red thrombus is a red blood cell-rich thrombus, which appears as an intramural mobile mass protruding into the lumen with high backscattering and attenuation. (Fig. 5A) A white thrombus is a platelet-rich thrombus that is defined as an intramural mass with homogeneous backscattering and low attenuation. (Fig. 5B) Because red thrombi could be misinterpreted as calcified nodules on OCT, the patient’s background history and lesion morphology (e.g., acute coronary syndrome, on hemodialysis) should be taken into accounts for their interpretation.
Fig. 5
Representative image of a red and white thrombus, and microvessel. A Red thrombus appears as an intramural mobile mass protruding into the lumen with a high backscattering and attenuation. B White thrombus appears as an intramural mass with homogeneous backscattering and low attenuation. C Microvessel appears as a no-signal tubuloluminal structure without a connection to the vessel lumen in multiple contiguous cross-sections
Cholesterol crystals: Cholesterol crystals on OCT might appear as a thin, linear region of high signal-intensity within a lipid-rich plaque. However, further histological validation data would be necessary for the accurate detection of cholesterol crystals.
Microvessels: A microvessel appears as a no-signal tubuloluminal structure without a connection to the vessel lumen. These microvessels usually have a sharply delineated border and can be followed in multiple contiguous cross-sections. (Fig. 5C) Owing to the limited penetration depth and axial resolution of OCT, the capability of OCT to reliably detect tiny microvessels in vulnerable atheromatous plaques merits future research. Recanalization of organized thrombus can be identified as multiple large channels, described as having “honeycomb-like appearance”, “swiss cheese appearance”, or “lotus root appearance”.
Layered plaque: After plaque rupture or plaque erosion in a coronary artery, a patient does not necessarily develop an acute coronary syndrome. If the degree of stenosis prior to rupture is low, thrombus formation may occur; however, in some cases, the event may not progress [18]. In such instances, the newly formed thrombus organizes and deposits connective tissue, primarily proteoglycans and type III collagen [19, 20], which appears as a band of high backscattered signal on OCT/OFDI. A previous histopathologic validation study reported good agreement between healed plaques observed in pathology and layered plaques seen on OCT [21]. Layered plaque is defined as a plaque with one or more layers of differing optical densities and a clear demarcation from the underlying components (Fig. 6).
Fig. 6
Representative image of a layered plaque. The double-headed arrow indicates a layer with different optical densities. A OCT image. B In the OFDI, there are three layers of different optical densities
Dissection: OCT is commonly employed to detect dissections after interventional stent implantation. The classification of dissections into five categories is recommended:
Intimal: Limited to the intima or plaque, and not extending to the media.
Medial: Extending into the media.
Adventitial: Extending through the external elastic membrane.
Intramural hematoma: An accumulation of flushing media within the medial space, displacing the internal elastic membrane inward and external elastic membrane outward.
Intra-stent: Separation of neointimal hyperplasia from stent struts, usually seen only after treatment of in-stent restenosis.
In-stent tissue protrusion: OCT’s high spatial resolution enables the detection and evaluation of tissue protrusions following stent implantation. It is recommended to classify in-stent tissue protrusion into three categories:
Smooth: Bowing of a plaque into the lumen between the stent struts without intimal disruption.
Disrupted fibrous tissue: Disruption of the underlying fibrous tissue protrusion into the lumen between the stent struts.
Irregular: Protruding the material with an irregular surface into the lumen between the stent struts.
Comments (0)