The adult surgeon is one of the fundamental stakeholders in ensuring the smooth and successful TOC. The results of this study were important to reflect the current TOC practices and challenges experienced by adult surgeons in Malaysia. The exploration of barriers was helpful in driving the direction of model development and implementation. Significantly, there was a proven need for a structured and algorithmic TOC model. The low number of referred cases managed by adult surgeons (1–5 cases in our study) revealed that TOC was not practiced widely among adult surgeons, which was consistent with the previously mentioned study that focused on pediatric surgeons in Malaysia [6].
With the advancement of technologies and the improvement of healthcare quality, the number of patients who achieve longer lifespans is expected to expand in the coming years. Pediatric surgery is a relatively new specialty in Malaysia. Starting from 2010, pediatric surgery is no longer a subspecialty of general surgery, i.e., medical graduates who are ambitious to specialize in pediatric surgery may enter the specialization program without the prerequisite of being a qualified adult general surgeon. This direct path may be favorable to most aspiring pediatric surgeons, but the concern of pediatric surgeons having less experience in handling adult surgical problems persisted.
The key factors influencing TOC in our study included increasing age, adult comorbidities, and patient independence.
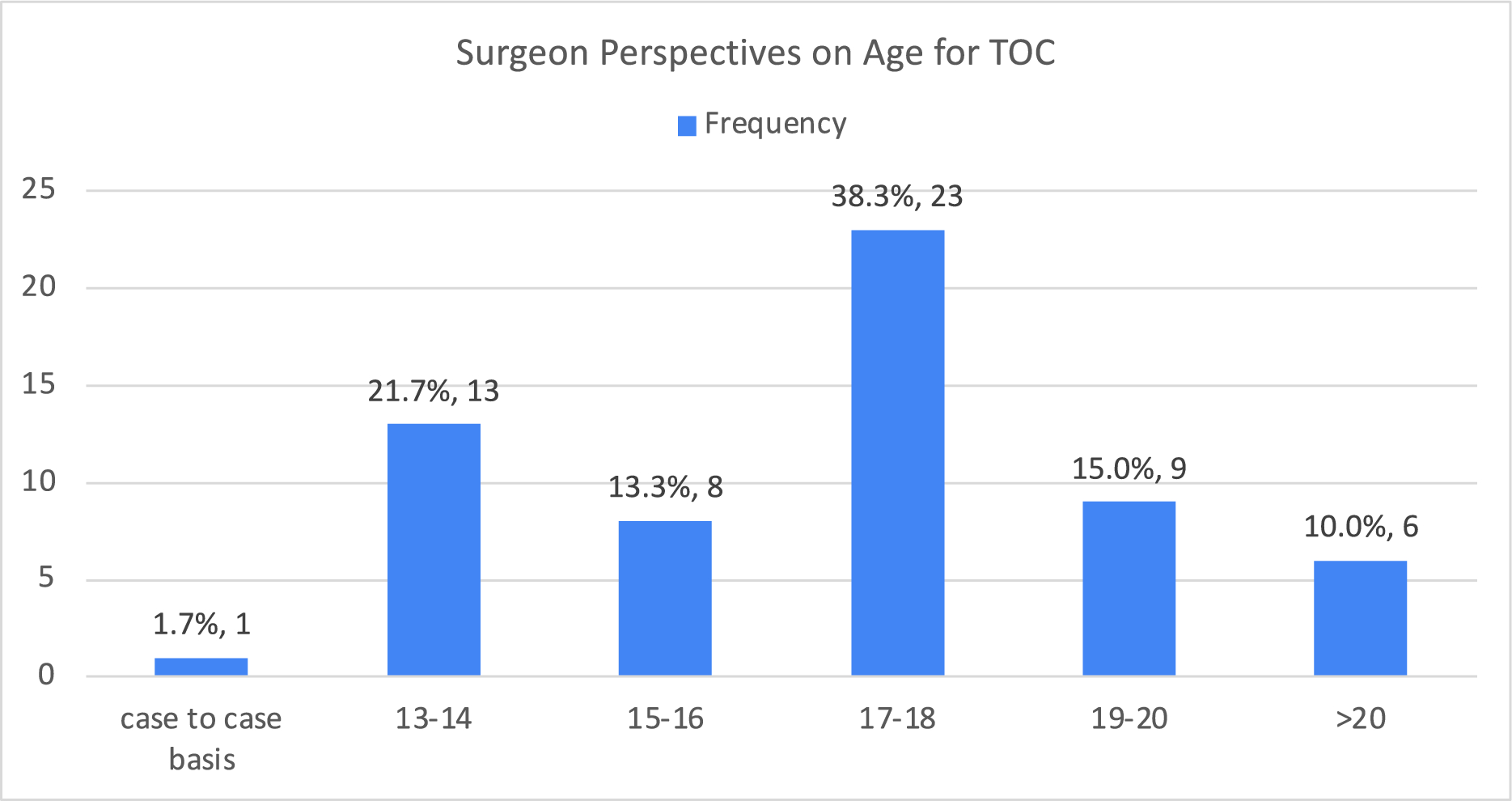
Age remained the main factor that necessitates the TOC based on surgeons’ experiences and opinions. Regarding one of the most commonly used TOC models—‘Ready, Steady, Go’, pediatric team would plan the transition in stages [2]. Young patients would start visiting the transition clinics, which consisted of both pediatric and adult teams, from 16 to 18 years old. This allowed formal communications and collaborations between surgeons and young patients might highlight their ongoing issues to the adult team [7]. Some studies suggested the start of the TOC in early adolescence [8]. From the respondents’ perspectives in our study, 17–18 years was deemed as the most appropriate age for the TOC. We acknowledged that the transition from pediatric to adult care was a gradual process that would occur at varying speeds depending on the conditions and individual circumstances. Our finding likely reflected the perspectives of adult general surgeons who participated in the study. However, evidence in the literature highlighted that transition planning should begin earlier, around the age of 12 years, to allow sufficient time for a gradual and effective transition process. This discrepancy might point to a gap in awareness among adult general surgeons about the challenges and nuances of transition, which were more commonly navigated by pediatricians and pediatric surgeons. In addition, this recommendation of age by adult surgeons in our study might be due to the local challenges, such as the shortage of experts in adolescent care and the lack of adolescent-friendly facilities [9].
The development of adult comorbidities was another paramount factor that demands TOC based on our study. The literature revealed that some patients moved on to lead a disease-free life post-surgery while some struggled with chronic symptoms, including physical and psychological disturbances, even after a successful surgery. Some disease-specific long-term morbidities included dysphagia in esophageal atresia, constipation in anorectal malformation and Hirschsprung’s disease, portal hypertension in biliary atresia, and pulmonary impairment in congenital diaphragmatic hernia [4]. There were also case series reporting the development of carcinomas in patients with a history of esophageal atresia and anorectal malformations in their 40s and 30s, respectively [10, 11]. This was concerning as regular follow-ups and disease surveillance might enable earlier detection and provide a better prognosis. Common adult comorbidities such as diabetes mellitus and hypertension were suggested to develop earlier in this patient population than in the general population [12, 13].
Almost all surgeons agreed that the TOC was beneficial to patient care and needed in Malaysia. This implied the support and interest of adult surgeons in improving the care of pediatric patients with complex surgical conditions. In addition, all surgeons claimed that the involvement of pediatric surgeons would lead to successful and smooth TOC. This aligned with the pediatric surgeons’ perspectives, which 84% of them expressed the obligation to provide consultations and care even after patients have been transferred to adult care [6].
In Malaysia, pediatric surgeons often continue to follow up with their patients into adulthood, as there is no formal handover process in place. Adopting and adapting TOC models from other countries might expedite the formation of an appropriate framework in Malaysia. The readiness of adolescents to navigate into the adult healthcare settings independently should be prioritized. The transitional care framework introduced by The North American Society for Paediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN), which eventually matched each adolescent with the adult care providers, might be studied and modified. This model ensured individualized and comprehensive care to patients [14].
Nevertheless, there were multiple barriers to TOC. In this study, adult surgeons perceived poor record management as the major barrier to a smooth TOC, followed by the absence of a proper guideline, lack of adult care providers familiar with pediatric surgical conditions, hospital policies, lack of TOC support staff, lack of awareness among healthcare providers, and ongoing active surgical problems in patients. By acknowledging and recognizing these barriers, they could be tackled accordingly.
There were some limitations to this study. The sample size of this study was small; it might not comprehensively represent adult surgeons from different subspecialties and different institutions. Besides, the responses were not stratified based on the specific congenital abnormalities managed by adult surgeons. Without this stratification, the specific referral pathway practiced by surgeons currently could not be identified and compared. Another limitation was that the questionnaire was not formally validated or assessed for internal reliability and consistency prior to its use. The robustness of the collected data and the generalizability of the findings might be reduced.
Following this study, which highlighted the need for a structured transition of care model in Malaysia, we recommended initiating deeper discussions between adult and pediatric surgeons. These discussions should aim to develop models such as combined clinics and multidisciplinary approaches to ensure a seamless TOC. A multidisciplinary team (MDT) might involve a core team (i.e., pediatric surgeons, adult surgeons, nursing, and imaging teams) and an extended team (i.e., anesthesiologist, psychologist/counselor, social workers, and nutritionist). This multidisciplinary approach serves to promote collaboration, create awareness among involved parties and bridge the gaps. Several issues that have to be addressed include the availability of resources (i.e., trained healthcare personnel, medical equipment, and country’s health expenditure), the acknowledgement of the need of TOC by each discipline involved, and the quantification of the need. The ideal model should be patient-centered, case-specific, and collaborative, ensuring that the unique needs of each patient are fulfilled.







Comments (0)