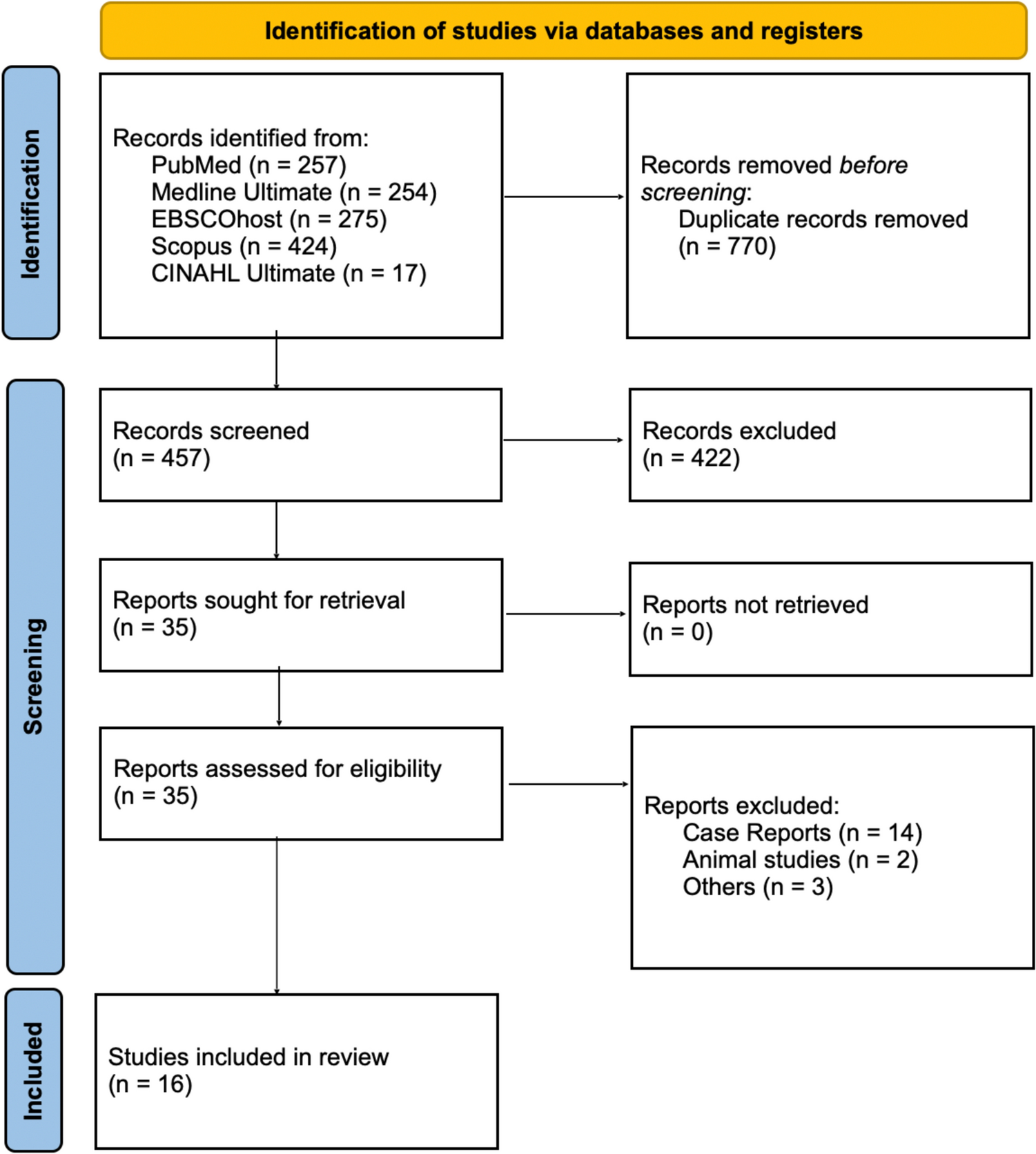
After a systematic literature search, only three articles met the inclusion criteria (Table 1 and Fig. 1).
Table 1 Data extracted from the systematic analysisNelson et al. conducted a cross-sectional study involving 66 patients who underwent oral mucosa graft urethroplasty (OMGU) procedures between 1992 and 2003 [8]. Out of 51 patients that could be traced, 43 patients agreed to participate (84%). The study instrument, consisting of 20 items, was a combination and modification of validated questionnaires. It included the American Urological Association (AUA) International Prostate Symptom Score (IPSS) index for Benign Prostatic Hyperplasia (BPH) to assess urinary function, supplemented by two additional items from previous studies to evaluate urinary spraying and urinary stream. Oral symptoms were also analyzed but were not included in our study. The assessment focused on satisfaction with urinary function, penile appearance, and surgical results. Mean age at the time of the study was 15.1 ± 11.2 years. Age categories were 11 years or younger (51%), 11–17 years (23%),18 years and older (26%). All patients were operated on before puberty. Complaints regarding urinary spraying were reported by 11 patients (26%), while 12 patients (28%) experienced problems with aiming the stream. In terms of the AUA symptom index score IPSS, the majority of patients (77%) had mild symptoms, with 16% reporting moderate symptoms, and 5% reporting severe symptoms.
Patients who had undergone OMGU after a previous failed urethral repair tended to have a worse IPSS. Overall satisfaction with urinary function was mixed, with 60% of patients feeling mostly satisfied or better. Urethral complications were common post-OMGU, with 22 patients (51%) requiring one or more additional procedures. Among these patients, five had meatal stenosis, six had urethral strictures, five had urethrocutaneous fistulas, and six had a combination of these problems.
In the retrospective study conducted by Figueroa et al., the medical records of 137 patients who underwent oral mucosa urethroplasty between 2000 and 2010 were examined [9]. Further analysis was conducted specifically on boys who underwent the first stage of the procedure before the age of 12 and had their last follow-up recorded after puberty. The data reviewed included demographic information, initial meatal location, quality of the graft before tubularization, flow rate, and complications. Out of the initial 137 patients, only 10 met the inclusion criteria for this study due to lack of agreement, missing follow-up data, or failure to meet the inclusion criteria. The mean age of patients at the time of surgery was 8 years old (range 5–11 years), with a mean follow-up period of 40.6 months (range 9–66 months). Among these patients, 5 had undergone a redo procedure following failed hypospadias correction using the urethral plate (TIP). Complications observed included one fistula and two cases of glandular dehiscence. The final position of the meatus was glandular in 9 patients and coronal in one. No cases of ventral curvature were reported by neither the patients nor their parents. The average maximum flow rate, as reported by the authors, was considered adequate for the patients’ age, with a mean of 25.7 ml/sec.
In the retrospective study conducted by Goyal et al., out of the initial cohort of 37 patients who underwent OMGU between 1994 and 2002, 30 patients were available for inclusion in the study [10]. Among these, 28 were categorized as post pubertal at the time of the study, while the remaining 2 were classified as peripubertal. Early surgical complications were observed in 10 patients, with the most common complications being fistula formation in 7 cases, urethral stricture in 2 cases, and a single case of tortuous urethra. In terms of long-term complications, one patient developed obstructive balanitis xerotica obliterans in the grafted urethra and 5 meatal stenosis.
Risk assessment ROBINS-I
Table 2 provides an overview of the risk of bias assessment for each included study using the ROBINS-I tool.
Table 2 Outcomes RoB analysis using ROBINS-I (7)Most bias occurs prior or after the intervention, whereas the intervention itself is without bias. The study of Figueroa et al. [9] lacked a control group, selection was unclear and the high percentage of participants excluded due to missing data raised critical risks of bias in these aspects. Despite these limitations, the study demonstrated low risk in the classification of interventions and deviations from intended interventions. Overall, this study’s risk of bias is assessed as serious. Similar to the previous study, the study of Goyal et al. [10] lacked a control group or comparison with other techniques introduces a serious risk of bias due to confounding. Furthermore, the use of non-validated questionnaires to assess outcomes and the method of retrospective assessment of files with different severity of hypospadias led to a serious risk of bias in outcome measurement. Despite the low risk of bias in the selection of participants and classification of interventions and that no deviations from intended interventions were documented nor missing data, the overall risk of bias in this study is serious. The last study, Nelson et al. [8], displayed an overall moderate risk of bias. There was moderate risk due to confounding and the lack of explicit information on participant selection and on the self-reported questionnaires for outcome measurement. On the other hand, the classification of interventions demonstrated a low risk of bias, with a clear description of the surgical techniques and deviations from intended interventions and missing data.







Comments (0)