The main finding of our study is that hepatoblastoma patients (>5 years old) have higher sAFP levels compared to HCC patients. High sAFP levels are a typical laboratory finding in hepatoblastoma and HCC patients [8, 11]. AFP is a glycoprotein that is normally produced by the yolk sac and fetal liver during pregnancy, and serum levels decline rapidly after birth due to suppression of AFP expression [12]. In our study, higher sAFP levels in hepatoblastoma may be explained by the fetal and/or embryonic origin of the tumor. Unlike hepatoblastoma, in HCC, the tumor tissue regains the ability to produce oncofetal protein as a result of complex genetic mechanisms that have not yet been fully elucidated [12]. To the best of our knowledge, there is no study comparing HCC and hepatoblastoma in terms of sAFP levels.
It is known that the sAFP levels are usually normal in fibrolamellar HCC and have a good prognosis compared to classical type HCC in adults [13]. However, Katzenstein et al. and Wahab et al. showed that fibrolamellar HCC may not be associated with a favorable prognosis in children, and elevated sAFP levels of up to 10% have been reported [14, 15]. Also, another study by McDonald et al. showed that 44% of adult fibrolamellar HCC patients have elevated sAFP levels and higher levels are associated with worse prognosis [13]. In our study, a fibrolamellar HCC patient with a high sAFP level developed multiple recurrent tumors after surgical resection, and liver transplantation was performed. In contrast to HCC, low sAFP levels at diagnosis (<100 ng/ml) are considered high risk in patients with hepatoblastoma and are mostly associated with small cell undifferentiated histologic type [11]. None of the patients in our cohort had low sAFP levels, which may be explained by epithelial or mixed histological type of all tumors.
In the literature, both hepatoblastoma and HCC patients had slight male predilection [16, 17]. Similarly, in our study, most of the patients were male in both groups.
The PRETEXT staging system is routinely used for staging, risk stratification, and determining surgical approach in children with primary hepatic malignancies [10, 18]. In our study, PRETEXT III (22%) and IV (66%) tumors were more common in the hepatoblastoma group. Hiyama et al. and Meyer et al. reported that PRETEXT stage IV has a rate of 15–23% in hepatoblastoma [19, 20]. In comparison to these results, we found that PRETEXT IV disease was more common in patients older than 5; however, it may not be possible to extrapolate this finding due to the small sample size. Consistent with the literature by D’Souza et al., PRETEXT I and II tumors were more frequent in the HCC group [21]. A recently published article by Rees et al. showed that HCC patients with predispositions tend to have smaller tumor size, lower PRETEXT stage, and less frequent tumor in vein [22]. This could be explained by surveillance imaging in children with predisposing factors. The two HCC patients with tyrosinemia in our study were detected at routine follow-up imaging and classified as PRETEXT I and II. Annotation factors including hepatic venous/vena cava inferior involvement (V), portal venous involvement (P), extrahepatic disease contiguous with the primary liver tumor (E), multifocal tumor (F), tumor rupture (R), involvement of the caudate lobe (C), lymph node metastasis (N), and distant metastasis (M) were associated with adverse prognosis [23]. The most common positive annotation factor was hepatic venous/vena cava inferior involvement in both groups (50% in the HCC group and 77% in the hepatoblastoma group). In addition, portal venous involvement and multifocal tumor were rare in HCC patients in our cohort when compared with the literature [24]).
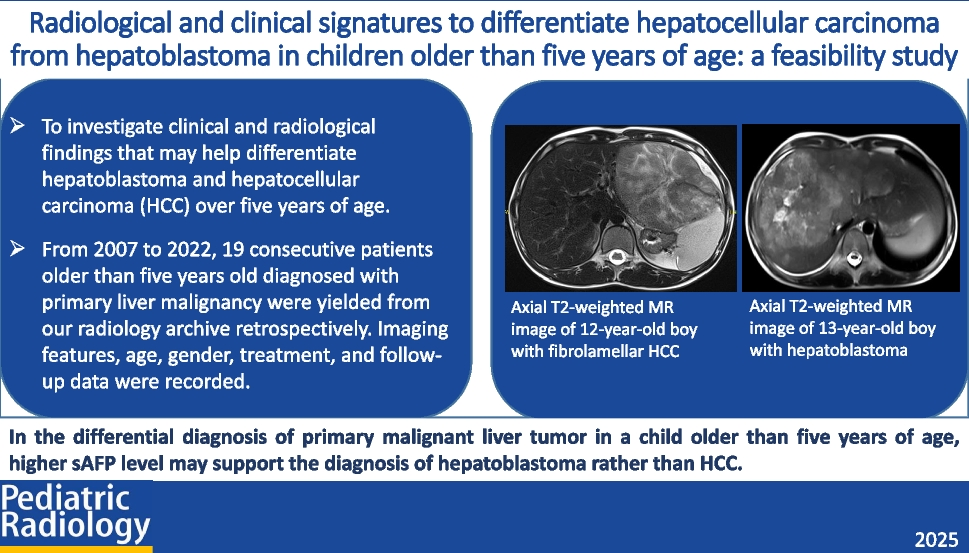
Liver Imaging Reporting and Data System (LI-RADS) provides a standardized lexicon for radiologic imaging and is commonly used to diagnose adult HCC. However, LI-RADS major criteria have a limited value in children due to low specificity and interobserver agreement (24). Similar to the results by Khanna et al., we found APHE 55%, non-peripheral washout 55%, and enhancing capsule 22% in the HCC group [25]. APHE and washout were not detected in any of the hepatoblastoma cases. Therefore, the LI-RADS major criteria, although nonspecific, may help distinguish these two tumors. Finally, we found a signal drop on dual-phase GRE T1-weighted images representing intralesional fat in three patients with hepatoblastoma. The presence of fat in a malignant liver lesion is considered a quite specific but insensitive imaging feature of HCC in adults [26]. However, intralesional fat is not a typical finding of either pediatric HCC or hepatoblastoma.
Our study has several limitations. First, due to the retrospective design and long time span of the study, not all imaging modalities were available for each patient, and the image acquisition technique varied widely. Second, although HCC and hepatoblastoma are rare tumors in children over 5 years old, the overall sample size was small. The lack of a similar previous study also prevented us from conducting a power analysis. Although tumor size and PRETEXT stages were higher in hepatoblastoma patients, these differences were not statistically significant, likely due to the limited sample size. Further definitive studies with larger patient groups are needed to identify clinical and radiological signatures that may be helpful in the differential diagnosis of primary malignant liver tumors in children over the age of 5 years old.
In conclusion, although hepatoblastoma is rare in patients over 5 years of age, it should be included in the differential diagnosis of radiologically malignant tumors beyond HCC. This study indicates that high AFP levels may serve as a laboratory finding to support the diagnosis of hepatoblastoma in this age group. These observations require confirmation from other cohorts.





Comments (0)