Most ADPKD patients (estimated as 95%) present with bilateral and diffuse distribution of the disease, while a minority have an atypical imaging pattern (Class 2 of Mayo Clinic Imaging Classification) [6]. Despite the achievements in the management of ADPKD patients, there are currently no strong predictors for disease progression in Class 2 ADPKD, mainly because of the lack of large population studies, which is also why the prevalence of this specific population is still not fully known. The incidence of Class 2 ADPKD patients in our cohort was consistent with other single-center published cohorts (5.4% vs 5–10%) [5]. A comparison of the patients’ characteristics between the Bologna cohort and the cohorts described in the literature can be found in Table 4.
Table 4 Comparison of clinical features in atypical ADPKD patients from our cohort and from cohorts described in the literature [3, 6, 13] Class 2 ADPKD patients need to be better characterized with regard to family history, genetics, and clinical features, like kidney function decline, urological events, hypertension, and extrarenal manifestations. As for family history, 75.0% of our population presented a positive family history, similar to what was reported for Class 1 patients [13]. These data aligned with some other reported cohorts [3,) (14,) (15], while in the Iliuta et al. [13] cohort, the prevalence of a positive family history was extremely low [3]. We evaluated all of our patients’ family members who were willing to undergo genetic testing and sonography to detect the presence of cystic disease. Many family members of our cohort had never been genetically tested, highlighting the possibility of missed diagnosis in cases of cystic kidney diseases regardless of progression to kidney failure. We believe that the high percentage of positive family history we found is indicative of the need for nephrological and genetic assessment of all family members of patients affected by this specific phenotype.
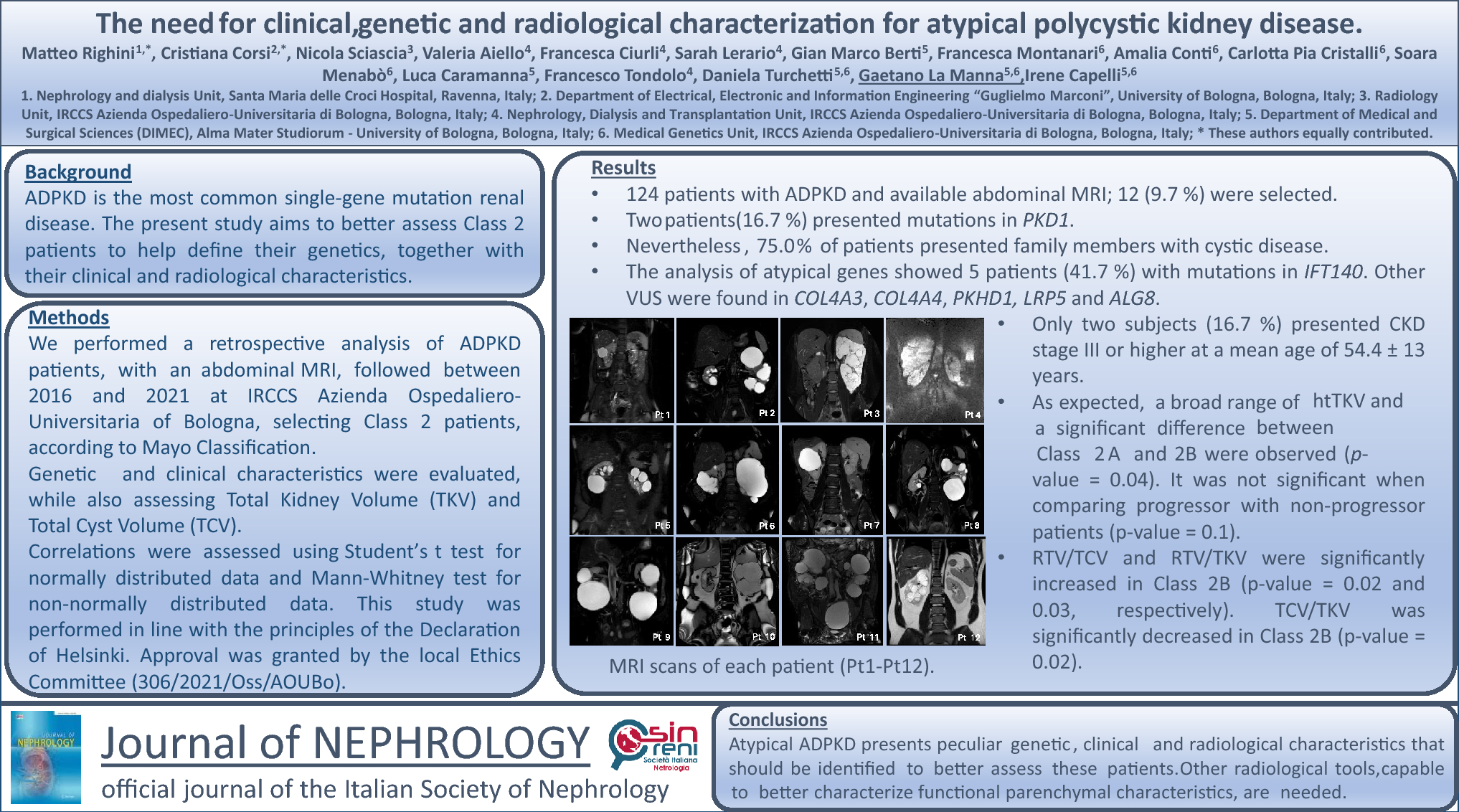
Among our cohort, 83.3% did not carry any mutation in the PKD1 or PKD2 genes. Two patients (16.7%) carried a PKD1 mutated gene: one subject had a non-truncating variant classified as likely pathogenic (NM_001009944.3: c.2180 T > C p. Leu727Pro), while the second one presented a variant of uncertain significance (NM_001009944.3: c.194 T > A p.Ile65Asn). In the study conducted by Iliuta et al. [14], 30.4% of Class 2 ADPKD patients presented a truncating PKD1 mutation, 30.4% had a PKD2 mutation and 39.2% did not present any variant. In our study, the percentage of typical mutated genes was much lower (16.7%). Thus, we decided to search for the involvement of other genes, as already suggested by other authors [16,17,18,19,20,21,22]. Broadening our analysis to a targeted resequencing approach led to the identification of pathogenic variants in IFT140, and variants of uncertain significance in COL4A4, COL4A3, PKHD1, LRP5 and ALG8. Despite this further analysis, a specific genetic diagnosis was still missing for three patients. It is possible that other genes, still unidentified may be involved. According to several studies, ADPKD shows high genetic complexity, thus attributing the correct diagnosis and providing adequate genetic counseling to affected patients and their families is mandatory [23, 24]. This concept clearly emerged from our study, as the extension of the genetic analyses to non-PKD1/PKD2 genes confirmed the diagnosis in five cases (41.7%), and described variants of uncertain significance in three cases (25.0%). Recent reports [25] described IFT140 in ADPKD-like phenotypes, including both kidney and liver cysts, and suggesting a link in > 1% of cases. The percentage of negative-PKD1/PKD2 patients in our cohort with a variant in IFT140 (41.7%) was higher than that reported in the literature (20%), even though the disease was generally mild, as expected.
Regarding the other mutated genes, as reported in the literature, the ones related to Alport syndrome (COL4A3, COL4A4) can be associated with kidney cysts. Gulati and colleagues observed that collagen IV gene mutations were present in a series of patients with bilateral kidney cysts, suggesting that type IV collagen mutations may be present in ADPKD patients without mutations in the PKD1 or PKD2 genes [16].With regard to PKHD1, although the perinatal manifestation is the most common form, later onset was also described in the literature [23]. ALG8 was another gene involved in the development of kidney and liver cysts, even though the severity of the disease was mild [22].
Regarding kidney function, progression has been reported as slower in these patients [3,4,5,6]. Determining the number of kidney cysts and the volume growth patterns may provide additional insights into the clinical management and treatment in ADPKD patients, as the growth in kidney volume directly stems from the increase in kidney cyst volume [26]. As described by Irazabal et al. [3], the only significant predictors for kidney function progression in Class 2 ADPKD patients are eGFR at baseline and atrophic vs non atrophic radiological presentation. In the literature, height-adjusted total kidney volume was observed to be the least predictive tool for Class 2 patients [5]. Neither height-adjusted total kidney volume nor the slope of total kidney volume resulted significant [26, 27], as opposed to Class 1 patients. We evaluated kidney function trend in our cohort, confirming the presence of mild kidney disease in our patients (only two subjects presented CKD stage III or higher, with a mean age of 54.4 ± 13 years). There were only two rapid progressors, according to the definition provided in the 2022 ERKNet Position Statement [28]. The absence of a trend towards severe progression, albeit in agreement with previous literature data, could also be related to the limited number of patients in our cohort. When assessing eGFR in Class 2A and Class 2B patients, our analysis did not find a significant difference in the eGFR (p value = 0.9) or in the eGFR slope (p value = 0.1).
In this study, we also aimed to evaluate total cyst volume. As already observed by Cadnapaphornchai and colleagues, total cyst volume assessment could be a useful tool in children with ADPKD [29]. Furthermore, in a longitudinal study conducted by Bae et al. [30], the authors used total cyst volume to describe the growth of cysts and kidneys over time. Despite using a different method to measure total cyst volume, our findings did not reveal any significant differences in either total cyst volume or residual tissue volume between patients with preserved or impaired kidney function, but a difference between Class 2A and 2B is highlighted (p value = 0.04). The significant increase in residual tissue volume/total cyst volume and residual tissue volume/total kidney volume and the significant reduction in total cyst volume/total kidney volume in Class 2B may imply the presence of a structural difference between the two classes of ADPKD, and warrant further validation in larger cohorts to link the structural aspect to functional behavior.
Extrarenal involvement and hypertension were present in a high percentage of cases in our cohort. In comparison, only Iliuta et al. [13] evaluated the presence of liver cysts, that were present in 87.0% of cases. This suggests the need to investigate the presence of extrarenal involvement in affected patients and in their family members, to better characterize the patients’ phenotype. Hypertension was present in more than 50% of cases, in line with other reports in typical ADPKD patients.
Conclusions
In conclusion, Class 2 ADPKD patients present genetic and clinical differences compared to Class 1 subjects. Two patients carried a likely pathogenic mutation and a variant of uncertain significance in the PKD1 gene. The research of a cystic phenotype in family members of affected subjects revealed significant cystic involvement with a more variable functional progression, thus suggesting the need for family screening. The decline in kidney function was observed to be slower. Extrarenal involvement and hypertension are frequent and are important issues that need to be assessed in affected patients.
Finally, residual tissue volume did not correlate with kidney function in Class 2 ADPKD patients. This result highlights that other imaging tools should be investigated in future research in order to understand kidney prognosis in Class 2 patients.







Comments (0)