
Remember me





We divided the drugs used for treating psychosis and agitation in subjects with AD into four classes: approved, off-label, repurposed, and novel compounds. In the off-label drug class, we included compounds approved for other clinical indications and previously tested for the treatment of agitation or psychosis in AD but that are no longer being actively tested for these indications. In the repurposed drug class, we included compounds that are approved for other clinical indications and are actively being tested in agitation or psychosis in AD. Tables 1 and 2 present the main ongoing clinical trials on drugs for the treatment of psychosis and agitation associated to AD. Figure 1 shows emerging drugs for agitation and psychosis in AD and their potential neurobiological pathways of action.
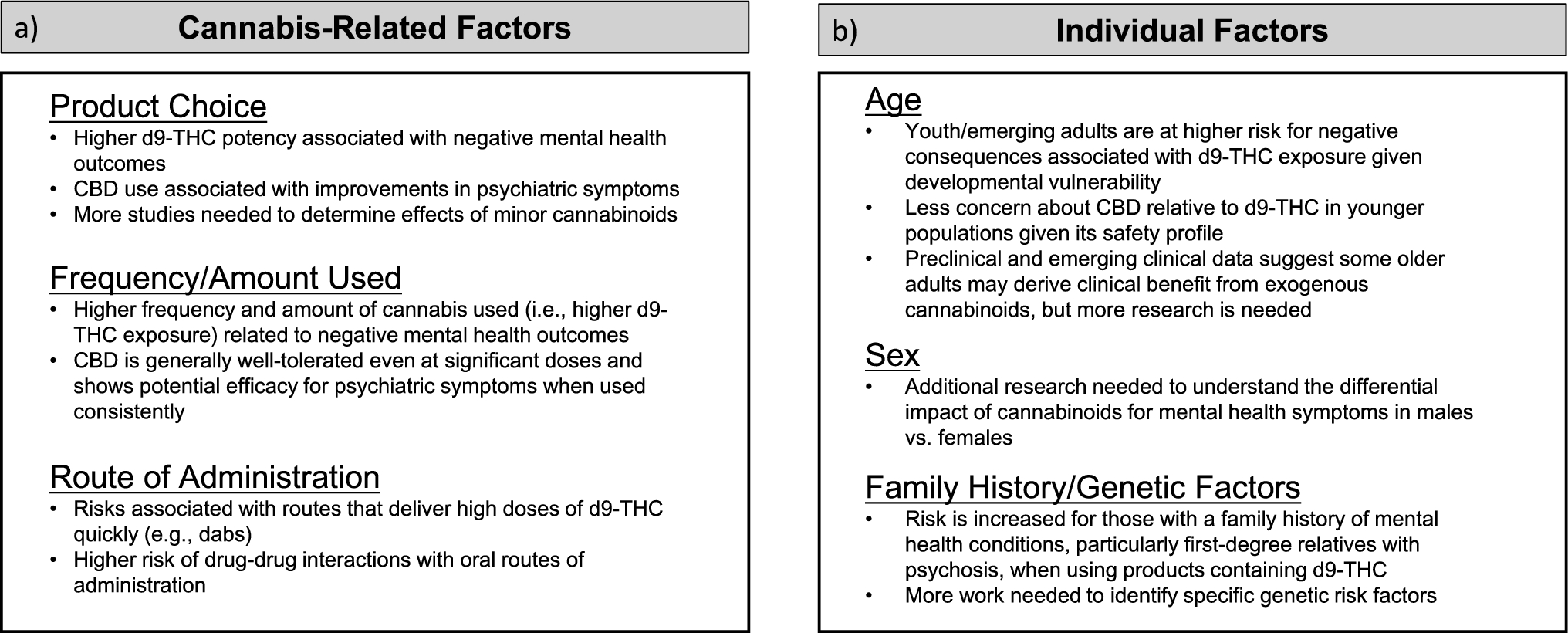
Table 1 Main ongoing clinical trials on drugs for the treatment of psychosis in Alzheimer’s diseaseTable 2 Main ongoing clinical trials on drugs for the treatment of agitation in Alzheimer’s diseaseFig. 1
Emerging drugs for agitation and psychosis in Alzheimer’s disease. A Schematic representation of potential neurotransmitter pathways involved in agitation and psychosis in AD. B Main pharmacological binding profiles of emergent drugs for agitation in AD. C Main pharmacological binding profiles of emergent drugs for psychosis in AD. 5-HT 5-hydroxytryptamine, 5-HT1A 5-hydroxytryptamine receptor 1A, 5-HT2A 5-hydroxytryptamine receptor 2A, 5-HT6 5-hydroxytryptamine receptor 6, α alpha adrenergic, α1 alpha-1 adrenergic receptor, α2 alpha-2 adrenergic receptor, CB cannabinoid receptor, D dopamine, D2 dopamine receptor D2, D3 dopamine receptor D3, M muscarinic, M1 muscarinic receptor M1, M4 muscarinic receptor M4, NET norepinephrine transporter, NMDA N-methyl-d-aspartate receptor, PDE10A phosphodiesterase 10A, SERT serotonin transporter, σ1 sigma 1 receptor. Figure created with BioRender.com
6.1 Approved Drugs for Agitation in AD6.1.1 BrexpiprazoleBrexpiprazole is a newer atypical antipsychotic and was recently approved by the FDA for the treatment of agitation associated to dementia due to AD. This atypical antipsychotic has the most favorable efficacy/risk profile, and this has been ascribed to its partial agonism of the serotonin 5-HT1A receptor and the dopamine D2 and D3 receptors [47]. Brexpiprazole has been approved also for schizophrenia and as adjunctive therapy in adult major depressive disorder (MDD). A first 12-week, double-blind, placebo-controlled study involved 433 participants in a care facility or community-based setting with diagnosis of probable AD (NINCDS-ADRDA criteria) and clinically significant agitation (Neuropsychiatric Inventory-Nursing Home, NPI-NH, ≥ 4) [48]. Cognitive impairment at baseline was quite wide assessed with Mini-Mental State Examination (MMSE, 5–22). The primary outcome measure of efficacy was the CMAI total score, while the secondary outcome was the Clinical Global Impression-Severity of Illness (CGI-S) modified for agitation. Patients were randomized in 1:1:1 ratio to fixed doses of brexpiprazole 2 mg/day, brexpiprazole 1 mg/day, or placebo, for 12 weeks. The study initially included a fourth treatment arm with brexpiprazole 0.5 mg/day, which was discontinued based on the evidence from other studies that the 0.5 mg/day dose was ineffective in older adults. At week 12, the 2 mg/day dose showed significant reductions in the CMAI total score compared with placebo (− 3.77 points; p = 0.040), while the 1 mg/day dose did not demonstrate significant difference from placebo. On the CGI-S scale, the 2 mg/day dose showed a nonsignificant trend compared with the placebo group. Adverse events in the 2 mg/day group were headache (9.3% versus 8.1% with placebo), insomnia (5.7% versus 4.4%), dizziness (5.7% versus 3.0%), and urinary tract infection (5.0% versus 1.5%). A second 12-week study involved 270 patients, who were randomized in 1:1 ratio to a flexible dose regimen of brexpiprazole (from 0.5 to 2 mg/day) or placebo [48]. At week 12, brexpiprazole did not show a statistically significant difference on the CMAI total score compared with placebo (− 2.34 points, p = 0.15) but a statistically significant reduction in the CGI-S score compared with placebo (− 0.31 points, p = 0.016). Adverse events among patients receiving brexpiprazole were headache (7.6% versus 12.4% with placebo) and somnolence (6.1% versus 3.6%) [48].
A further 12-week, double-blind, placebo-controlled, fixed-dose study involving 345 patients with agitation in AD in a care facility or community-based setting evaluated brexpiprazole at doses of 2 or 3 mg/day [49]. The primary outcome measure of efficacy was the CMAI total score. Patients receiving brexpiprazole (n = 225) showed a statistically significant greater improvement than those taking placebo (n = 116) in the CMAI total score (− 17.3 points, p = 0.003) with a Cohen d effect size of 0.35. No adverse events had an incidence of 5% or more in the brexpiprazole group or a higher incidence than in the placebo group; 5.3% versus 4.3% of patients discontinued the study because of adverse events in the brexpiprazole and placebo group, respectively [49].
A recent 10-week, double-blind study evaluated brexpiprazole (1 mg/day, n = 112; 2 mg/day, n = 149) versus placebo (n = 149) in AD patients with agitation, defined according to IPA criteria and a score of ≥ 4 on the NPI-NH or NPI scales, with three or more instances of verbal or physical aggression in the 2 weeks prior to the study. The primary endpoint was CMAI score. Completion rates were 74.1%, 68.5%, and 77.9%, respectively. Both brexpiprazole groups showed significant reductions in CMAI scores compared with placebo (2 mg: − 7.2, p < 0.0001; 1 mg: − 3.7, p = 0.0175). Reductions in the 2 mg group appeared by week 4, continuing through week 10; the 1 mg group showed improvement by week 8. The incidence of adverse events was higher in the 2 mg group (84.6%) compared with the 1 mg group (76.8%) and placebo (73.8%). Two deaths in the 1 mg group were deemed unrelated to treatment [50].
Brexpiprazole carries a “boxed warning” for an increased risk of death, found to be four times higher in treated patients compared with placebo in pivotal trials and consistent with other atypical antipsychotics in older patients with dementia, as stated by the FDA [12]. During three randomized phase 3 trials, seven patients died: six (0.9%) in the brexpiprazole groups and one (0.3%) in the placebo groups; these deaths were considered unrelated to brexpiprazole treatment by the investigators [48, 49]. Additional two deaths occurred in the latest brexpiprazole trial, also reported as unrelated to the drug [50]. Other concerns include urinary tract infections, somnolence, insomnia, and cardiovascular events. No serious cerebrovascular adverse events have been reported, but patients and clinicians should be aware of this potential risk [12].
6.2 Off-Label Drugs for Psychosis and Agitation in AD6.2.1 Atypical AntipsychoticsThe role of atypical antipsychotics (AAPs) in treating psychosis and agitation in AD has been thoroughly reviewed [8, 9, 51]. Risperidone is approved for short-term treatment of severe NPSs (agitation/aggression) in the European Union, United Kingdom, Australia, and Canada, among other countries, but not in the United States. AAPs show overall modest efficacy in treating NPSs [52], with slight superiority over placebo for risperidone and aripiprazole in both agitation and psychosis [51, 53, 54]. Quetiapine and olanzapine are commonly prescribed, though evidence supporting their use is limited [52]. Antipsychotics pose significant risks, including extrapyramidal symptoms, falls, strokes, and increased mortality [11]. A metaanalysis found a higher mortality risk in patients with dementia taking antipsychotics versus placebo (3.5% versus 2.3%, odds ratio 1.54; 95% CI 1.06–2.23; p = 0.02) [55]. A recent population-based study linked antipsychotic use to a broader range of serious adverse outcomes, such as pneumonia, acute kidney injury, venous thromboembolism, fractures, and myocardial infarction, especially soon after treatment initiation [56]. AAPs may have different risk profiles, with risperidone and olanzapine linked to cardiovascular and extrapyramidal risks, while quetiapine is associated with sedation [57]. However, no AAP has a clear safety advantage regarding mortality [57]. Thus, individualized risk–benefit assessments are critical when prescribing these drugs to patients with dementia. AAPs should be used at the lowest effective dose for the shortest duration, as chronic use increases mortality [58]. Guidelines recommend discussing potential risks and benefits with patients (if clinically feasible) and caregivers, assessing efficacy after a 4-week trial, and tapering the drug within 4 months if symptoms improve, unless relapse occurs [10]. Ineffective drugs should be discontinued before starting new psychoactive treatments [52]. Clinical judgment is key to minimizing antipsychotic use, optimizing nonpharmacological approaches, and supporting caregiver management of agitation and psychosis. Screening for cardiovascular risk may also reduce morbidity and mortality [9].
6.2.2 Cholinesterase InhibitorsA recent review of 12 RCTs conducted in AD found that cholinesterase inhibitors (ChEIs), such as donepezil, rivastigmine, and galantamine, attenuated the severity of both delusions and hallucinations in AD, but with quite a small effect size (Cohen’s d < 0.20) and dubious clinical significance [59]. Similarly, ChEIs have shown little to no efficacy in reducing agitation in AD patients [20, 60]. Nevertheless, proposed algorithms for the management of NPSs suggest ChEI treatment as they may delay the onset of these symptoms and reduce the need for other psychotropic drugs [10, 54].
6.2.3 MemantineMemantine is a noncompetitive N-methyl-d-aspartate (NMDA) receptor antagonist approved for the treatment of moderate-to-severe AD. Pooled and post hoc analyses showed a modest positive effect of memantine on agitation and aggression [61] and on agitation and psychosis [62] in AD patients after 6 and 3 months of treatment, respectively. In both studies, NPSs were assessed using the NPI. However, RCTs specifically designed to test the efficacy of memantine in NPSs did not produce clinically meaningful results [63]. Interestingly, memantine in addition to antipsychotics appeared to improve negative symptoms in patients with schizophrenia [64], and it is currently being tested for this indication in the AMEND trial (NCT04789915).
6.2.4 AntidepressantsEvidence from a limited number of RCTs and metaanalyses suggests that selective serotonin reuptake inhibitors (SSRIs) may modestly improve agitation and overall NPSs in AD dementia [65, 66]. A recent network metaanalysis comparing SSRIs (sertraline, citalopram, and fluoxetine) with other antidepressants (trazodone and mirtazapine) found that only citalopram showed some benefit with acceptable safety [67]. The best evidence supporting the use of citalopram for agitation in AD comes from the CitAD study [68], a double-blind placebo-controlled trial, where 186 patients received either citalopram (up to 30 mg/day) or placebo for 9 weeks along with a psychosocial intervention. Citalopram improved agitation, psychosis, anxiety, and irritability but caused prolonged QTc and reduced MMSE scores, suggesting that its cognitive and cardiac side effects may limit its practical use. A subanalysis of this study found that citalopram had additional benefit on the frequency of irritability, anxiety, delusions, and hallucinations [69]. Owing to cardiac side effects, the FDA recommends a maximum daily dose of 20 mg for patients aged over 65 years [54].
Other antidepressants have been studied for agitation in AD. A post hoc analysis of a negative study on mirtazapine in 218 patients with depression suggested a positive trend in reducing median NPI scores [70], but in the 12-week SYMBAD study, mirtazapine (up to 45 mg/day) did not reduce agitation (measured with CMAI score) [71]. Limited evidence suggests that the sedating effect of trazodone may help reduce irritability and agitation in patients with dementia, and its use on a PRN basis for acute agitation has been advocated [63].
Concerning psychosis in AD, evidence supporting antidepressants is weak [66]. A network metaanalysis found no significant difference between citalopram, sertraline, trazodone, and placebo in reducing psychotic symptoms, but the smaller number of trials and sample sizes for antidepressants may have reduced the statistical power of each comparison [72].
6.2.5 LithiumLithium, a mood stabilizer used for bipolar mania, has been explored for disruptive behaviors and psychotic symptoms in dementia. A case series of six patients with dementia, agitation, and psychosis unresponsive to antipsychotics showed behavioral improvement with low-dose lithium (300–600 mg daily) and minor side effects [73]. However, a 12-week, double-blind, placebo-controlled study in 77 AD patients found no significant reduction in NPI agitation/aggression scores with lithium (150-600 mg/day) compared with placebo, although there was improvement on the Clinical Global Impression and Young Mania Rating Scale [74]. Lithium did not show significant safety issues, but larger trials are needed to validate these findings.
6.2.6 PrazosinPrazosin, a selective α-1 adrenergic receptor antagonist, was originally used to treat hypertension and reduce distressing dreams in post-traumatic stress disorder (PTSD). In the AD brain, degeneration of adrenergic neurons in the locus coeruleus leads to compensatory increases in norepinephrine and α-1 receptors [75]. Studies in a transgenic mouse model of AD have shown that prazosin prevents memory deterioration [76] and counteracts Aβ-induced vasoconstriction [77]. Prazosin has been proposed for treating agitation in AD [78]. An initial 8-week, double-blind, placebo-controlled study in 24 AD patients with agitation found that 6 mg/day of prazosin reduced NPI scores compared with placebo [79]. However, two subsequent small 12-week trials (NCT01126099 and PEACE-AD trial) and a 10-week study in PTSD patients at risk for AD (NCT03221751) showed no significant results.
6.3 Repurposed Drugs for Psychosis in AD6.3.1 PimavanserinPimavanserin is a serotonin-receptor modulator that acts primarily as a selective 5-HT2A inverse agonist, approved by the FDA for the treatment of Parkinson’s disease (PD) psychosis [52]. It does not bind to D2 dopamine receptors and has a potentially lower mortality risk than conventional atypical antipsychotics used for this indication [80]. In a 6-week trial involving 199 subjects with PD psychosis allocated (1:1) to receive pimavanserin 40 mg per day or matched placebo, subjects taking pimavanserin had a significant mean decrease in the PD-adapted scale for assessment of positive symptoms (SAPS-PD) than those receiving placebo (− 5.79 versus − 2.73 points, respectively) [81]. Interestingly, the subgroup of patients with cognitive impairment (n = 50) had a wider difference from baseline in the psychosis score than the cognitively unimpaired patients (n = 135) [82]. In a 12-week, double-blind, placebo-controlled trial involving 181 subjects with AD-related psychosis (randomly assigned 1:1 to drug or placebo), pimavanserin (two 17 mg tablets daily) significantly decreased the mean psychosis score (NPI-NH) compared with placebo at week 6, but not at week 12 [83]. In a double-blind, randomized, placebo-controlled discontinuation trial (HARMONY trial) involving 392 patients with psychosis related to AD, PD dementia, dementia with Lewy bodies, frontotemporal dementia, or vascular dementia, pimavanserin responders at week 12 (n = 217) were randomly assigned in 1:1 ratio to continue receiving pimavanserin or to receive placebo for additional 26 weeks [84]. The trial was stopped early for efficacy: a relapse of psychosis occurred in 12 of 95 patients (13%) in the pimavanserin group and in 28 of 99 (28%) in the placebo group (p = 0.005). Headache, constipation, urinary tract infection, and asymptomatic QT prolongation were the main adverse events occurring in subjects taking pimavanserin [84]. Despite these encouraging results, in August 2022, the FDA rejected the approval of pimavanserin for the treatment of psychosis due to AD, claiming that these were mainly due to the subgroup of patients with PD dementia. The FDA also raised concerns over the “limitations in the interpretability” of the results of the phase 2 study in 181 individuals with AD-related psychosis. It is presently unclear whether the sponsor of the drug (Acadia) will perform additional studies on pimavanserin in AD.
6.3.2 Xanomeline-TrospiumKarXT is the combination of the M1/M4-preferring muscarinic receptor agonist xanomeline with trospium chloride, a peripherally acting muscarinic receptor antagonist that reduces peripheral cholinergic effects of xanomeline [85]. Xanomeline-trospium has been successfully tested in individuals with schizophrenia and has recently been approved by the FDA for this indication, on the basis of two pivotal phase III trials, EMERGENT-2 and EMERGENT-3 [86]. These results support xanomeline-trospium as the first new antipsychotic medication without D2 dopamine receptor-blocking activity [85]. Since 2022, KarXT is being evaluated for treatment of psychosis in subjects with AD in two phase 3 trials. The ADEPT-1 study (NCT05511363) is enrolling 380 AD patients with history of moderate to severe hallucinations or delusions. The study is evaluating a wide range of doses and is being conducted according to a withdrawal design, with all patients receiving the drug combination for 12 weeks, followed by randomization to drug or placebo for an additional 26 weeks. The primary outcome measure of efficacy is time to relapse of psychosis symptoms, while the secondary objective is time from randomization to discontinuation for any reason. The ADEPT-2 study (NCT06126224) will enroll 400 participants and will evaluate the efficacy of KarXT at 12 weeks on psychiatric symptoms. Dosing will be titrated to a maximum of 200 mg xanomeline/20 mg trospium daily. A 1-year, open-label safety extension was planned to begin in 2023 and end in 2025.
6.4 Repurposed Drugs for Agitation in AD6.4.1 Dextromethorphan-BupropionAXS-05 is a fixed-dose combination of dextromethorphan and bupropion, approved by the FDA for the treatment of major depressive disorder [87] and currently being investigated for agitation in AD. Dextromethorphan acts as a noncompetitive NMDA receptor antagonist, a sigma-1 receptor agonist, and a serotonin-norepinephrine reuptake inhibitor. Bupropion is a norepinephrine and dopamine reuptake inhibitor, as well as a nicotinic acetylcholine receptor antagonist; it increases dextromethorphan plasma concentrations by slowing its metabolism [87].
The ADVANCE study (NCT03226522), a 5-week, double-blind, placebo-controlled trial, was the first study comparing the efficacy of AXS-05, bupropion, and placebo in 366 individuals with probable AD and agitation. Participants were randomized to receive AXS-05 (titrated to a final dose of 45 mg dextromethorphan/105 mg bupropion twice daily, n = 159), bupropion (105 mg twice daily, n = 49), or placebo (n = 158), using change in the CMAI as the primary outcome measure. AXS-05 significantly reduced CMAI score by − 15.4 points compared with bupropion alone (− 10.0; p < 0.001) or placebo (− 11.5; p = 0.010) [31]. The most frequent side effects of AXS-05 were somnolence and dizziness; no serious adverse events, sedation, or detrimental effects on cognition, as assessed with the MMSE, were observed [88]. Another double-blind, placebo-controlled study (ACCORD, NCT04797715) tested AXS-05 for agitation in 178 patients with AD according to a relapse-prevention trial design. Initially, all patients received AXS-05 for 9 weeks. At the end of this period, responders (n = 108; defined as ≥ 30% improvement from baseline in the CMAI total score and Patient Global Impression of Change score improvements ≤ 3 lasting ≥ 4 consecutive weeks) were randomized in 1:1 ratio to drug or placebo for up to 26 weeks [89]. The primary outcome measure of efficacy was time from randomization to relapse of agitation. AXS-05 significantly delayed the time to relapse of agitation symptoms compared with placebo (hazard ratio = 0.275; p = 0.014) and decreased relapse rate compared with placebo (7.5% versus 25.9%, p = 0.018). Compared with placebo, no significant sedation or cognitive decline were reported in patients taking AXS-05 [89]. A further 5-week, double-blind, placebo-controlled study (ADVANCE-2, NCT05557409) is presently enrolling 350 people with twice-daily AXS-05, with an optional 6-month open-label extension. The primary outcome of efficacy of this study is change in CMAI. Completion of the study is planned for June 2025.
6.4.2 DexmedetomidineDexmedetomidine is an α2-adrenergic receptor agonist approved in intravenous form for procedural sedation and anesthesia. A sublingual formulation (BXCL501) of the drug has also been approved by the FDA for the treatment of acute agitation associated with schizophrenia and bipolar disorder, on the basis of results of the SERENITY I and II trials [90]. BXCL501 shows a r
Comments (0)