
Remember me
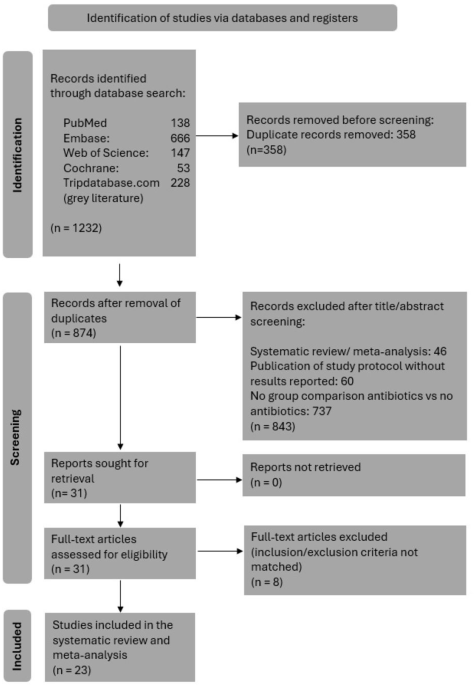
There were 9136 eligible patients with a new diagnosis of mHSPC during the study period (Fig. S1), of which 4937 were included in the comparative analysis: 315 who received upfront treatment with APA + ADT, 1181 treated with ENZ + ADT, 1760 treated with AAP + ADT, 432 treated with DTX + ADT, and 1249 treated with ADT alone (Table 1). As only 62 patients received upfront DARO + ADT + DTX with limited follow-up, this group was not included in the analysis.
Table 1 Demographic and clinical characteristics of patients at baseline, by starting treatment.The mean age of patients was similar in each group (range of means 69.0 to 74.4 years). Compared to patients who received an ARPI + ADT or ADT alone, patients who received upfront DTX + ADT tended to have more visceral metastases (16.9% versus 4.2–8.5%). CCI scores were distributed similarly between groups. The most frequently occurring comorbidities in each treatment group were diabetes (8.8 to 12.7% of patients), congestive heart failure (5.4% to 6.6%), and renal disease (4.9 to 10.2%).
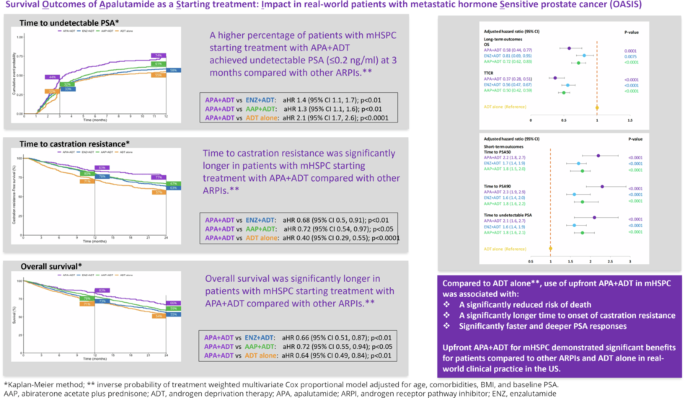
Short-term outcomesTime to PSA50 and PSA90At the 3-month timepoint, 70% of patients who initiated APA + ADT had reached PSA50 versus 60% in the ENZ + ADT, 59% in the AAP + ADT group, 58% in the DTX + ADT group, and 32% in the ADT alone group (Fig. 1). At month 12, 79% of patients in the APA + ADT group had reached PSA50 versus 77%, 74%, 72%, and 52%, respectively. The median time to PSA50 was 2.13 months in the APA + ADT group, 2.33 months in the ENZ + ADT group, 2.52 months in the AAP + ADT group, 2.30 months in the DTX + ADT group, and 8.98 months in the ADT alone group (Table S1). Adjusted HRs for the likelihood of reaching PSA50 at any time were significantly higher in all groups compared to ADT alone (Fig. 2). The likelihood of reaching PSA50 was significantly higher for APA + ADT compared with ENZ + ADT (aHR 1.4 [95% CI 1.2–1.7]), AAP + ADT (aHR 1.3 [95% CI 1.1–1.6]), DTX + ADT (aHR 1.7 [95% CI 1.4–2.1]), and ADT alone (aHR 2.4 [95% CI 1.9–2.9]) (Table 2).
Fig. 1: Time to PSA50, PSA90 and undetectable PSA ( < 0.2 ng/ml) by starting treatment in patients with mHSPC – Kaplan-Meier method.
AAP abiraterone acetate plus prednisone, ADT androgen deprivation therapy, APA apalutamide, DTX docetaxel, ENZ enzalutamide, mHSCP metastatic hormone-sensitive prostate cancer, PSA50/PSA90 50%/90% decline in PSA from baseline, Undetectable PSA, ≤0.2 ng/ml.
Fig. 2: Multivariate Cox regression model* results for hazard ratios by starting treatment group in patients with mHSPC; ARPIs + ADT as compared to ADT alone.
AAP abiraterone acetate plus prednisone, ADT androgen deprivation therapy, APA apalutamide, DTX docetaxel, ENZ enzalutamide, mHSCP metastatic hormone-sensitive prostate cancer, OS overall survival, PSA50/PSA90 50%/90% decline in PSA from baseline, TTCR time to castration resistance, Undetectable PSA, ≤0.2 ng/ml. *Adjusted for age, comorbidities, BMI and baseline PSA level.
Table 2 Pair-wise comparisons assessing outcomes in patients starting on APA + ADT compared with other treatments—adjusteda multivariate Cox regression using the IPTW method.Similar findings were observed for PSA90. At 3 months, 49% of patients initiated on APA + ADT had reached PSA90 versus 38% in the ENZ + ADT group, 37% in the AAP + ADT group, 28% in the DTX + ADT group, and 15% in the ADT alone group (Fig. 1). At month 12, the percentages were 66%, 61%, 57%, 48%, and 36%, in the respective groups, and the median time to PSA90 was 3.08 months, 4.82 months, 4.62 months, 13.54 months, and was not reached for ADT alone (Table S1). Adjusted HRs for the likelihood of reaching PSA90 at any time were significantly higher in the ARPI + ADT groups compared to ADT alone (Fig. 2). The likelihood of reaching PSA90 was significantly higher for APA + ADT compared with ENZ + ADT (aHR 1.5 [95% CI 1.2–1.8]), AAP + ADT (aHR 1.3 [95% CI 1.1–1.6]), DXT + ADT (aHR 2.5 [95% CI 1.9–3.3] and ADT alone (aHR 2.4 [95% CI 1.9–3.1]) (Table 2).
Time to undetectable PSA ( ≤ 0.2 ng/ml)At 3 months, 44% of patients who initiated APA + ADT had undetectable PSA versus 32% in the ENZ + ADT group, 33% in the AAP + ADT group, 32% in the DTX + ADT group, and 20% in the ADT alone group (Fig. 1). At month 12, the percentages were 74%, 61%, 58%, 55, and 41%, in the respective groups, and the median time to undetectable PSA was 3.44 months, 6.30 months, 5.15 months, 22.62 months, and 6.89 months (Table S1). Adjusted HRs for the likelihood of reaching undetectable PSA were significantly higher in the ARPI + ADT groups compared to ADT alone (Fig. 2). The likelihood of reaching undetectable PSA was significantly higher for APA + ADT compared with ENZ + ADT (aHR 1.4 [95% CI 1.1–1.7]), AAP + ADT (aHR 1.3 [95% CI 1.1–1.6]), DTX + ADT (aHR 2.0 [95% CI 1.5–2.6]) and ADT alone (aHR 2.1 [95% CI 1.7–2.6]) (Table 2).
Long-term outcomesOverall survivalAt 24 months, 66% of patients who initiated APA + ADT were alive, versus 55% in the ENZ + ADT group, 59% in the AAP + ADT group, 42% in the DTX + ADT group, and 54% in the ADT alone group (Fig. 3). Median OS was not reached in the APA + ADT group, and was 28.56 months, 34.52 months, 17.18 months, and 26.79 months in the respective groups (Table S1). There was a significantly reduced risk of death in all ARPI + ADT groups compared to ADT alone. The risk of death was significantly higher in the DTX + ADT group than the ADT alone group (Fig. 2). Adjusted HRs [95% CI] for the risk of death were significantly lower in the APA + ADT group compared with ENZ + ADT (0.66 [0.51–0.87]), AAP + ADT (0.72 [0.55–0.94]), DTX + ADT (0.38 [0.28–0.52]) and ADT alone (0.64 [0.49–0.84]) (Table 2).
Fig. 3: Time to castration-resistance and overall survival by starting treatment in mHSPC – Kaplan-Meier method.
AAP abiraterone acetate plus prednisone, ADT androgen deprivation therapy, APA apalutamide, DTX docetaxel, ENZ enzalutamide, mHSCP metastatic hormone-sensitive prostate cancer.
Approximately 40% of patients in each group had a missing baseline ECOG PS. We evaluated OS in patients with known ECOG PS (0–1 or ≥2) versus those with an unknown score. OS in patients with an unknown score strongly resembled that in patients with ECOG PS 0–1 (p = 0.86) (Fig. S2), suggesting that ECOG PS was not an important confounding factor in our study.
Time to castration resistanceAt the 12-month timepoint, 83% of patients who started treatment with APA + ADT continued to be hormone sensitive versus 78% in the ENZ + ADT group, 80% in the AAP group, 57% in the DTX + ADT group, and 72% in the ADT alone group (Fig. 3). At 24 months the percentages were 77%, 63%, 67%, 32%, and 57%, respectively. The median TTCR was not reached in the APA + ADT group, and was 43.64 months in the ENZ + ADT group, 54.39 months in the AAP group, 15.05 in the DTX + ADT group, and 34.52 months in the ADT alone group (Table S1). The TTCR was significantly longer in the ARPI + ADT groups compared to ADT alone (Fig. 2). Adjusted HRs [95% CI] showed significantly longer TTCR when the starting treatment was with APA + ADT compared with ENZ + ADT (0.68 [0.50–0.91]), AAP + ADT (0.72 [0.54–0.97]), DTX + ADT (0.32 [0.23–0.44]), and ADT alone (0.40 [0.29–0.55]) (Table 2).
Comments (0)