
Remember me
Dear Editor,
Contact allergy is an exaggerated reaction of the individual’s immune system following exposure to low molecular weight chemicals triggering cell-mediated immunity.1
The term polysensitisation(syn.: polyvalent sensitisation, multiple contact allergies) describes sensitisation to more than one allergen verified by appropriate tests (e.g. skin prick test, specific immunoglobulin E [IgE] assays and epicutaneous patch testing).1
In India, there is a paucity of studies focused on polysensitivity. The main purpose of this study was to identify the common allergens involved, observe the patterns of monosensitisation and polysensitisation in allergic contact dermatitis (ACD) cases using the Indian standard series (ISS) and provide a review on polysensitivity.
A retrospective analytical study was done from 2015 to 2020 in the department of dermatology, JSS medical college, JSSAHER, Mysore. Clinically suspicious cases of ACD at any site irrespective of age and sex were subjected to patch testing using Indian Standard Series (ISS) with 20 allergens approved by Contact and Occupational Dermatitis Forum of India (CODFI). We used International Contact Dermatitis Research Group (ICDRG) criteria to identify the positive allergens in our study: 1+ erythema, infiltration and papules; 2+ vesicles; and 3+ vesicles coalescing to form bullae. Readings were taken on days two, four and seven. The comparison was done based on age, sex, site of eczema and allergens involved in monosensitivity and polysensitivity.
History, clinical presentation and outcome of patch test results and type of allergen were considered for relevancy. Among 182 patients, patch tests of 164 (89.61%) patients were relevant.
A total of 348 cases of ACD were included. Patch testing was positive in 182 patients (52.6%), single positivity in 114 (62.6%) and polysensitivity in 68 patients (37.1%). Positivity was seen more commonly in adults (19-64 years) [n=163 (89.6%)], followed by geriatric (>65 years) patients [n=11 (6%)] and adolescents (10-18 years) [n=8 (4.4%)]. Positivity to patch tests were slightly more in females [n=92 (50.5%)] compared to males [n=90 (49.5%)]. The most common sites involved in polysensitivity were both hands and feet [n=72 (39.6%)], followed by exclusive foot involvement [n=45(24.7%)] and generalised eczema [n=30 (16.5%)] [Table 1]. Polysensitivity to two, three and four allergens were seen in 45 (66.1%), 17 (25%) and 4 (5.8%) patients, respectively. There was one (1.5%) patient who had polysensitivity to five allergens and one (1.5%) to seven allergens [Figure 1].
Table 1: Frequency of monosensitivity and polysensitivity among the different sites involved in eczema
Site of eczema Monosensitivity Polysensitivity Hand-feet eczema 39(54.2%) 33(45.8%) Hand eczema 15(68.2%) 7(31.8%) Feet eczema 29(64.4%) 16(35.6%) Leg eczema 1 (100%) 0 Generalised eczema 30(71.4%) 12(28.6%)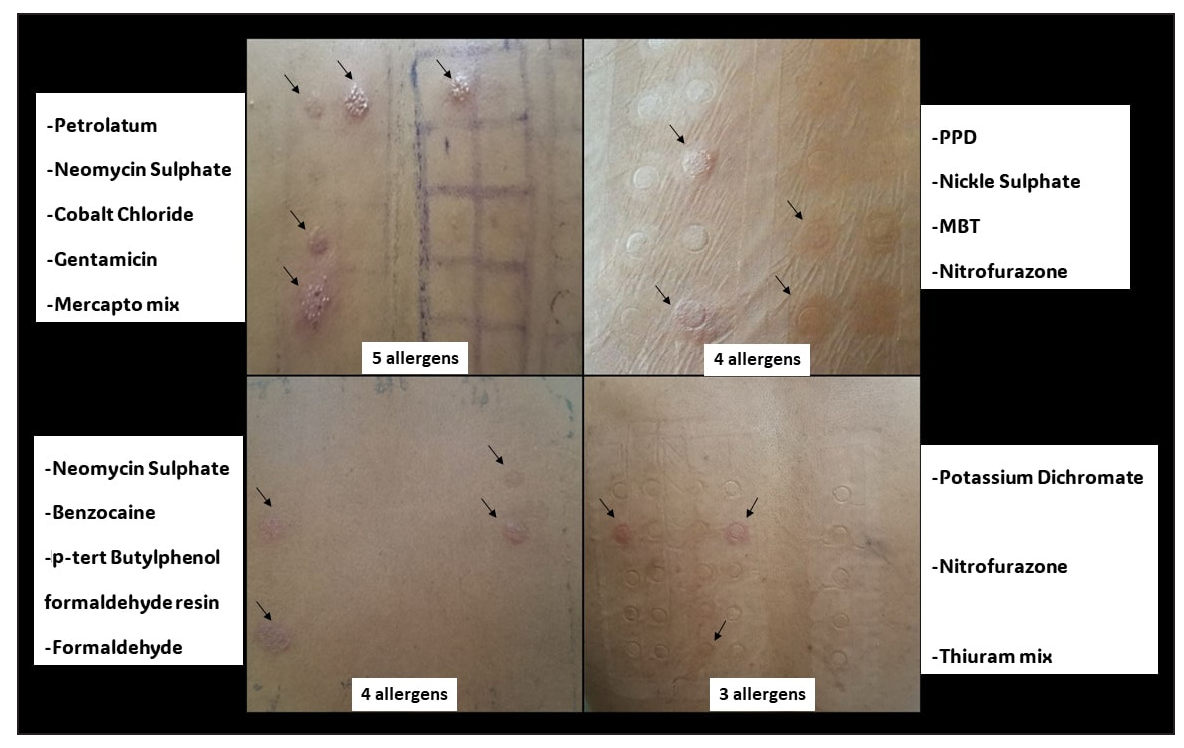
Export to PPT
We noted that polysensitivity was commonly seen with potassium dichromate and cobalt chloride among nine patients in hand-feet eczema; potassium dichromate, cobalt chloride and nickel sulphate among two patients in hand eczema; mercapto mix and 2-mercaptobenzothiazole (MBT) in five patients with feet eczema. We did not find polysensitivity among leg eczema cases and no allergens showed any common trend in generalised eczema.
There is ambiguity in the definition of polysensitisation. Few authors consider it to be a positive reaction to two or more allergens and few consider three or more allergens.1 Positive patch test results to two or more allergens were considered as polysensitivity in this study. Monosensitivity was seen more commonly with females [n=65 (70.7%)], whereas polysensitivity was seen more in males [n=41 (45.6%)]. Among different occupations, farmers [n=28(63.6%)] showed the most polysensitivity and housewives [n=35 (79.5%)] showed the highest rates of monosenstivity. There was no statistically significant difference with regard to age, duration of eczema and site of eczema among patients with monosensitivity and polysensitivity. The three prinicipal allergens in monosensitivity are nickel sulphate, potassium dichromate and paraphenyldiamine. Potassium dichromate, cobalt chloride; potassium dichromate, nickel sulphate; potassium dichromate, cobalt chloride, nickel sulphate; mercapto mix, 2-mercaptobenzothiozole are the three common allergen combinations involved in polysensitivity [Table 2]. Among the sites involved, patch tests in hand-feet eczema 35(48.6%) showed maximum polysensitivity.
Table 2: Summary of frequency of the most common allergens involved in monosensitivity and polysensitivity
Allergens Polysensitivity Monosensitivity Potassium dichromate, cobalt chloride 10 (14.7%) Potassium dichromate, nickel sulphate 10 (14.7%) Potassium dichromate, cobalt chloride, nickel sulphate 5 (7.4%) Mercapto mix, 2-mercaptobenzothiozole 5 (7.4%) Nickel sulphate 42 (36.8%) Potassium dichromate 32 (28.1%) Paraphenylidinediamine 22 (19.3%) Others 38 18Mahajan et al.2 observed that polysensitivity occurs due to concurrent exposure to allergens eliciting multiple positive patch test reactions from exposures to multiple allergens, non-specific hyper-reactivity or as cross- reactions between tested allergens. It is observed commonly for metals (nickel sulphate, cobalt chloride and potassium dichromate), rubber chemicals (mercapto mix, thiuram mix and monobenzothiazole (MBT), paraphenylenediamine (PPD) and parabens, compositae plants and some fragrances and Balsam of Peru. We observed a similar pattern.
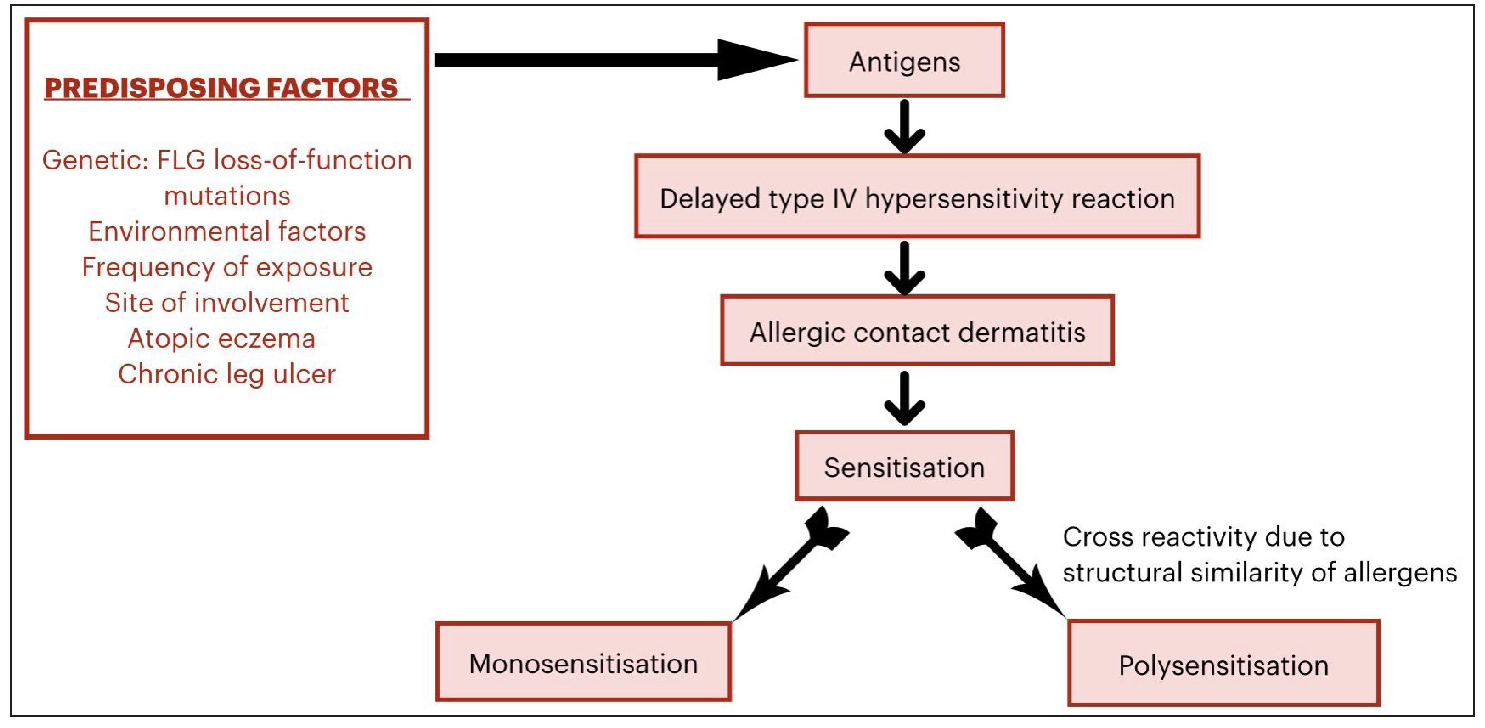
Distinguishing between true polysensitivity or angry back3 or excited skin syndrome or false positive reaction is necessary. Repeat patch testing can be performed. The reactions decrease by 40–60% in polysensitivity and 80% in angry back syndrome.4 The predisposing factors5-6 and pathogenesis of multiple contact allergies are depicted in Figure 2.
Export to PPT
A detailed assessment and personalised approach is required to manage the individual’s allergic triggers, aiming to reduce exposure to these allergens in the future and avoid cross reactions.
To conclude, 90% of the patch tests were clinically relevant. Polysensitivity was seen mostly in men among farmers, whereas monosensitivity was seen in women among homemakers. Nickel sulphate and potassium dichromate were common denominators in both polysensitivity and monosensitivity. On the contrary, paraphenyldiamine was more frequently observed with monosensitivity and cobalt chloride with polysensitivity.
Comments (0)