Study design and ethics
This is a single-center, single-blind, prospective cohort study. Ethical approval was granted by the Institutional Review Board of Jiangsu Provincial Cancer Hospital (2023 Ke-Fast 079; November 28, 2023). This study was registered with the Chinese Clinical Trial Registry (ChiCTR2300078510). Written informed consent was obtained from all participants. The study procedures adhered to the ethical standards of the responsible committee on human experimentation (Institutional or regional) and the Declaration of Helsinki (1975, revised 2013). This clinical trial was conducted from December 2023 to March 2024.
Participants
Adult patients aged 18–65 years, with American Society of Anesthesiologists (ASA) physical status I to III, who were scheduled for elective radical hysterectomy, were screened for eligibility. The exposed group exposed to NACT with a regimen of paclitaxel and platinum-based agents. Two chemotherapy regimens were used: paclitaxel (135–175 mg/m2) administered as a continuous intravenous infusion, and either cisplatin (75 mg/m2) or carboplatin (AUC = 5) administered as intraperitoneal injections. Both regimens were administered every 3 weeks. A radical hysterectomy was performed one week after the completion of 3 cycles of treatment. The non-exposed group consisted of patients who had not exposed to any baseline treatments, including immunotherapy, radiotherapy, or chemotherapy.
The exclusion criteria were as follows: (I) a history of severe neurological and psychiatric disorders, including dementia or Parkinson's disease; (II) a history of cranial trauma or brain surgery within the past three months; (III) severe asthma or allergies; (IV) significant anemia; (V) preoperative use of sedative-hypnotics or anticholinergics, as well as within 72 h postoperatively; (VI) abnormal liver or kidney function; specifically, liver dysfunction was identified by aspartate aminotransferase (AST) and alanine aminotransferase (ALT) levels exceeding 1.5 times the upper limit of normal, while kidney dysfunction was indicated by serum creatinine (Cr) levels ≥ 1.5 times the upper limit of normal; (VII) rhinitis that affects the sense of smell; (VIII) experiencing colds at the time of testing and the presence of other malignant tumors.
Inclusion and blinding
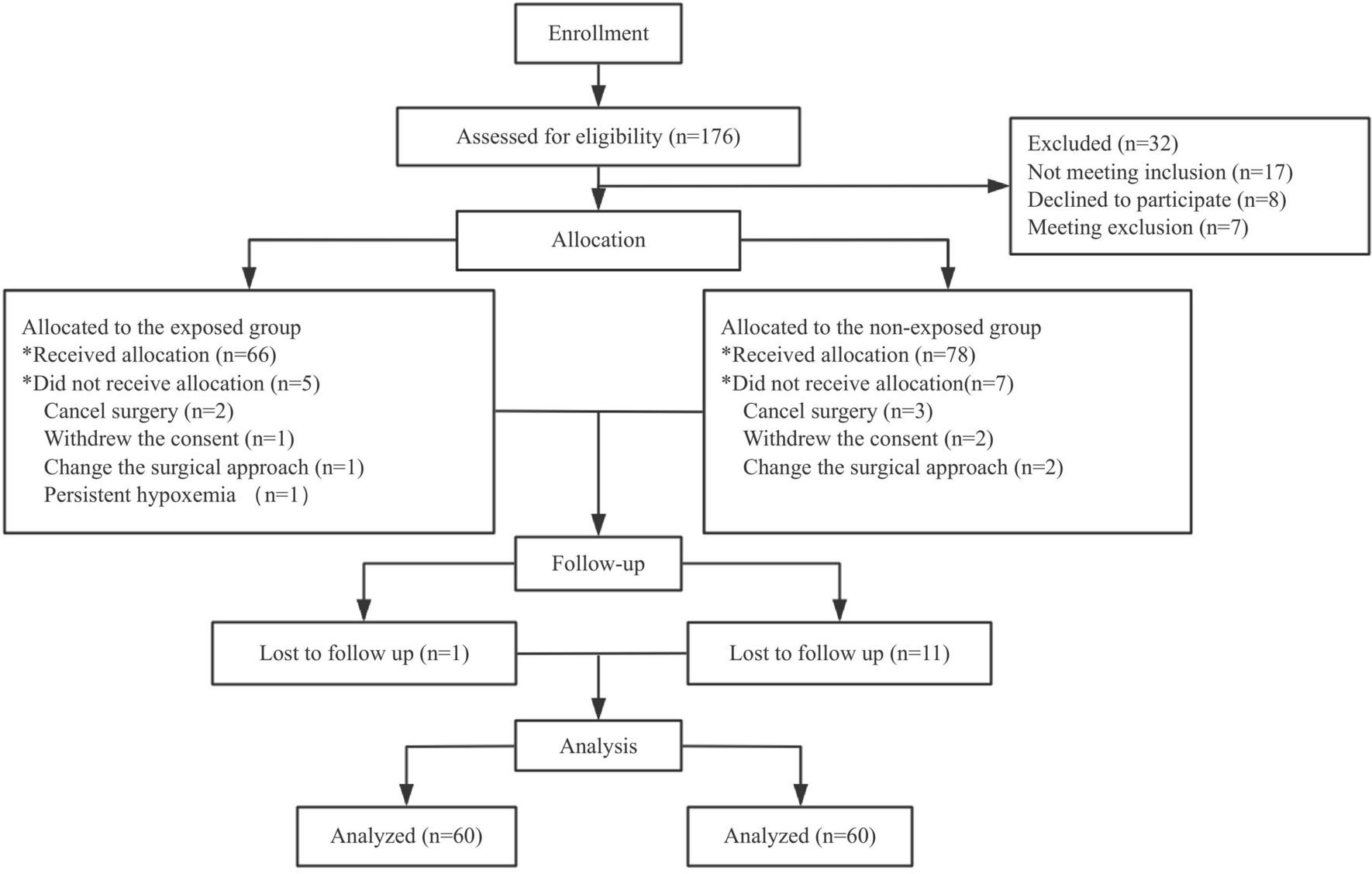
Eligible patients were evaluated by the investigators on the day prior to surgery. They were categorized into two groups: those who exposed to NACT, referred to as the exposed group, and those who did not, known as the non-exposed group. This categorization followed a 1:1 ratio. Both groups underwent the same anesthesia management during the surgery. Data collection occurred one day before the surgery and continued for three days postoperatively. The study utilized a single-blind design, whereby all relevant information was gathered by data collection personnel who were unaware of the allocation scheme. While the subjects and medical staff were informed of the allocation, only the investigators involved in follow-up and statistical analyses were blinded to the group assignments.
Anesthesia management
Patients did not receive any medication before the operation. Patients were monitored using Standard ASA parameters, including invasive radial artery blood pressure, electrocardiography, capnography, and pulse oximetry. Anesthesia was induced intravenously with midazolam (0.03–0.05 mg/kg), propofol (1.5–2.0 mg/kg), sufentanil (0.3–0.5 μg/kg), and rocuronium (0.6–0.9 mg/kg). Endotracheal intubation was performed for respiratory support. Anesthesia was maintained with a continuous intraoperative infusion of propofol (4–6 mg/kg/h), remifentanil (6–12 μg/kg/h), rocuronium (600 ug/kg/h), and dexmedetomidine (0.2 ug/kg/h), without the use of sevoflurane. All patients received the same protective ventilation strategy: PCV-VG mode with a tidal volume of 6–8 ml/kg, FiO2 of 60%, PEEP of 5cmH2O, a respiratory rate of 12–14 breaths/min, an inspiration/expiration ratio of 1:2, and a PETCO2 maintained between 35 to 45 mmHg). Intraoperative adjustments were made by modulating respiratory parameters to maintain SpO2 at ≥ 95%. Intraoperative anesthesia depth was monitored with Sedline and maintained within the range of 25–50. Mean arterial pressure was maintained within ± 20% of the baseline value during surgery, with vasopressor drugs administered as needed. Intravenous ephedrine was administered to patients with hypotension, defined as a systolic blood pressure less than 80% of the baseline value or below 90 mmHg). Atropine (0.5 mg) was administered if the heart rate fell below 40 beats/min. Intraoperative temperature was maintained at ≥ 36℃ using thermal blankets.
After the surgical procedure, patients were transferred to the post-anesthesia care unit for recovery. The endotracheal tube was removed once the patient was fully awake, had stable circulation, restored swallowing reflex, normal tidal volume, and minute ventilation, and had airway secretions successfully aspirated. Atropine and neostigmine were administered as needed to negate any residual neuromuscular blockade. Patients were permitted to be discharged to the ward once their Alderete score exceeded 9.
For the first 48 h after surgery, all patients received routine patient-controlled intravenous analgesia, which consisted of flurbiprofen axetil (100 mg) and dezocine (50 mg) diluted in 100 ml of normal saline. The infusion pump delivered a continuous basal rate of 1.5–2.0 ml/h, along with bolus doses of 1.0 ml and a 15-min lock-out period. Postoperative analgesia was monitored, and corrective actions, such as adjusting the analgesic pump settings or adding tramadol or oxycodone, were taken if the Numeric Rating Scale (NRS) score was 3 or higher.
Outcome assessments and testing
The primary outcome was the incidence of POD within 3 days after surgery. POD was assessed on postoperative day 1 (POD1), day 2 (POD2), and day 3 (POD3) using the Confusion Assessment Method (CAM) or the Confusion Assessment Method of the Intensive Care Unit (CAM-ICU). POD was defined as the occurrence of POD on any of the three days following surgery.
The secondary outcomes included the predictive value of OD for POD, postoperative nausea and vomiting (PONV), pain assessed by the NRS on POD1, POD2, POD3, and the length of hospitalization. PONV was defined as nausea and vomiting occurring within 24 h after surgery. Cognitive evaluation was conducted using the MoCA. Researchers assessed frailty using the Fatigue Resistance Ambulation, Illness and Loss of Weight Index (FRAIL), anxiety using the General Anxiety Disorder-7 (GAD-7), depression using the Patient Health Questionnaire-9 items (PHQ-9), and life capability using the Activities of Daily Living (ADL) scale on POD-1. Additionally, the olfactory assessment was performed qualitatively using an olfactory test wax block with 12 flavors (Jinhaimo Olfactory Disorder Auxiliary Diagnosis Card, Production Lot Number: 20230701, Jiangsu Parkinsense Biotech Co., Ltd). OD was defined as the inability to identify fewer than 8 out of odors in the olfactory test.
Other study parameters included preoperative diagnosis, gender, age, BMI, educational level, complications (such as hypertension, diabetes, and coronary heart disease), smoking status, alcohol consumption, operation duration, anesthesia duration, fluid infusion, blood loss, and the frequency of remedial analgesia.
Statistical analysis
Based on our pilot study, the sample size was determined by analyzing the prevalence of POD in the two groups. From preliminary data, we estimated an incidence of 28% in the exposed group and 4.7% in the non-exposed group. To achieve a statistical power of 90% with a two-sided significance level of 0.05, and maintaining a 1:1 ratio between the two groups, a total of 96 patients was needed for the study. The sample size calculation was conducted using Fisher’s Exact Test for Two Proportions in PASS 2021 software. To account for a potential 20% loss to follow-up or withdrawals of consent, we aimed to include 58 patients in the exposed group and 58 in the non-exposed group, bringing the total to 116 patients.
Statistical analysis and plotting were performed using SPSS version 27.0 and R version 4.4.0. The normality of the data distribution was assessed using the Shapiro–Wilk test and the Q-Q plot. Normally distributed variables were presented as mean ± standard deviation. Non-normally distributed variables were reported as median (IQR) and analyzed using the Kruskal–Wallis test. Categorical variables were expressed as counts (percentage) and compared using the Chi-square test or Fisher exact test, as appropriate. The authors considered a p value of < 0.05 (two-tailed) statistically significant. A 3-node restricted cubic spline plot was used to assess the potential non-linear relationship between the MoCA scores (represented by continuous variables) and the olfactory test scores (represented by continuous variables). Univariate and multivariate logistic regression analyses were performed to identify risk factors for POD. The study planned to include 12 potential confounding factors in the univariate analysis. The classification variable assignments for the binary logistics regression analysis were as follows: NACT (0 = No, 1 = Yes); OD (0 = No, 1 = Yes); Depression (0 = No, 1 = Yes); Education level (0 = Primary school and below, 1 = Junior high school and high school, 2 = University and above); Preoperative cognitive function (0 = Normal, 1 = Mild cognitive dysfunction, 2 = Moderate cognitive dysfunction); Frailty status (0 = Normal, 1 = Pre-frailty, 2 = Frailty). Variables with a p value < 0.05 in the univariate regression analysis were included in the multivariate logistic regression analysis. For multivariable analysis, such as multiple regression, logistic regression, and factor analysis, the rules of thumb were often adopted that the sample size should be 5, 10, or 20 times the number of variables. For 12 predictors, a sample size of 60 might be acceptable, and a sample size of 120 would meet the most stringent rule of thumb. The ROC curve for OD (represented by categorical variables) as a predictor of POD was plotted. The AUC was calculated, along with the sensitivity and specificity of the prediction.






Comments (0)