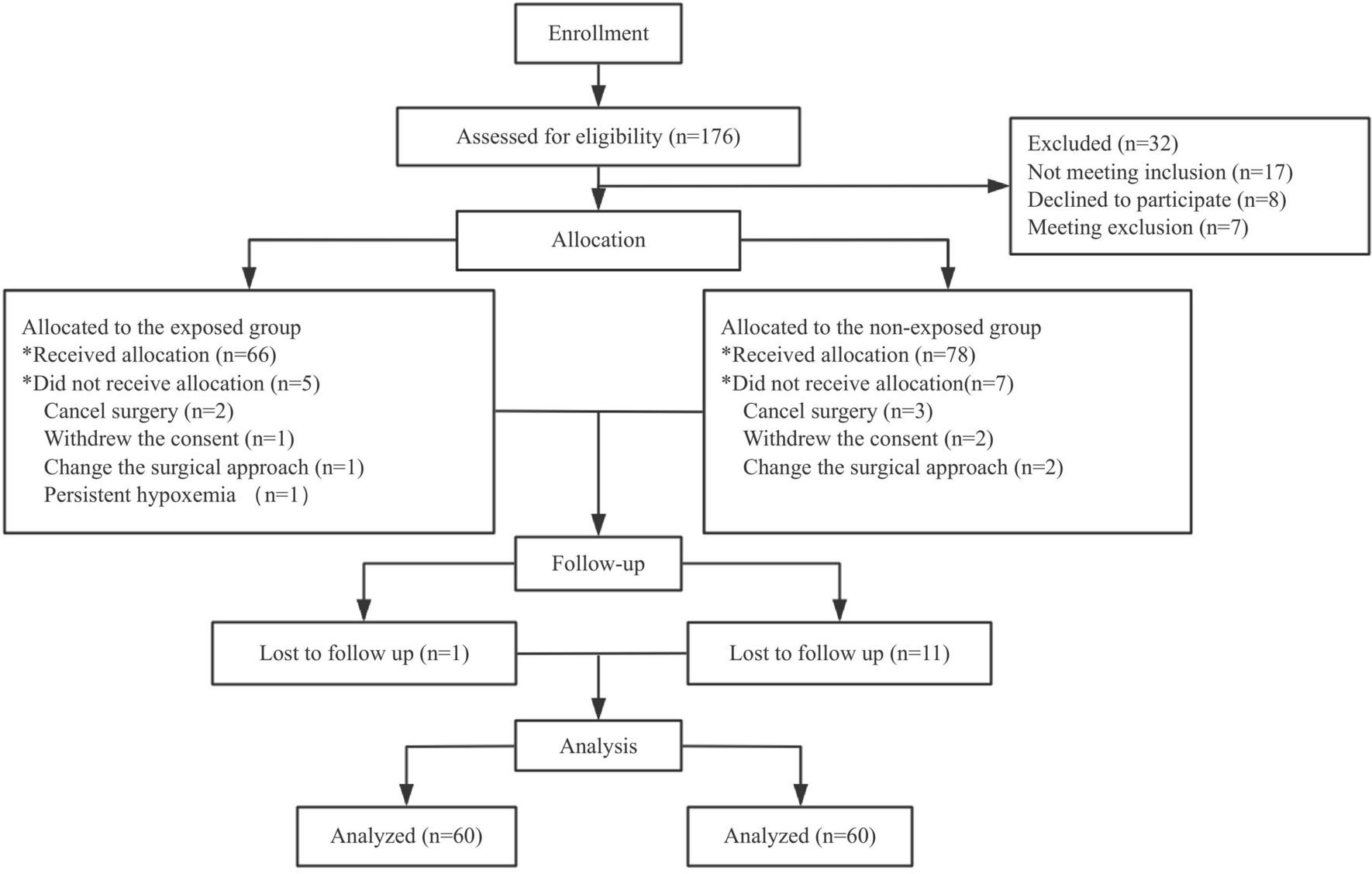
The research involved the analysis of data from the National Clinical Registry for Covid-19, which, included approximately 51,544 patients enrolled till 31st August 2023, who tested positive for the SARS-CoV-2 virus and were hospitalized across 42 hospitals in India. The primary focus of this study was to evaluate the hazard associated with all-cause mortality across various types of cancer when co-affected with COVID-19 within 30 days of hospital admission in comparison to other comorbidities and No Comorbidity. Additionally, the study aimed to compare the demographic and clinical characteristics of patients with different categories of cancer.
In this study, the most common cancers reported in males were gastrointestinal, followed by genitourinary and lung cancers. In females, breast cancer was most common, followed by genitourinary cancers. These findings are consistent with national cancer reports in India, which identify lung, mouth, oesophagus, stomach, and nasopharynx as the most common cancers in males, and genitourinary and breast cancers as the most common in females (Sathishkumar et al. 2022; Mathur 2020). The distribution of cancer cases across geographic zones in our registry showed heterogeneity, with the highest representation from North India, followed by Central and East India. While our findings align with national figures in terms of heterogeneous representation of cases, they differ from the magnitude and proportion of cancer cases reported by hospital-based cancer registries nationwide. These registries indicate the highest cancer burden in Central India, followed by the North East Zone. This discrepancy may be attributed to the design of our registry, whose initial mission was to focused on COVID-19 cases and considered designated COVID-19 hospitals. These hospitals might or might not have been to serve as the centres for cancer referrals (Mathur 2020).
There was significant difference in requirement of ICU and Organ Support across various categories of cancer with proportion of patients requiring support was highest among solid cancer (14.9%) while minimum among no form of cancer (10.46%). A study conducted in Chicago reported an ICU admission rate of 17.6%, figures that align with our findings. Also, there was no significant difference in distribution of requirement of supportive oxygen therapy and Invasive mechanical ventilation among Various categories of cancer. This observation contrasts with data from Brazil, which indicated a high usage of invasive mechanical ventilation (IMV) among cancer patients (Caruso et al. 2021). There has been ongoing debate about the relatively low rates of ICU admission and IMV use among cancer patients with COVID-19 (Mechanical Ventilation Rates and in Oncology Patients with COVID-19 – Consult QD. 2021). This could be attributed to the fact that many cancer patients in our study may have had advanced cancer and were primarily receiving palliative care when they contracted COVID-19, leading to a disproportionately low rate of ICU admission and IMV utilization. Additionally, it’s worth noting that the median age of our cancer cohort ranged between 56 to 60 years, which may have contributed to the lower proportion of ICU admissions and organ support, as older cancer patients with reduced life expectancy might have been triaged due to the global shortage of ICU beds during the peak of the pandemic (Azoulay et al. 2011).
In this study, there was no discernible difference in the occurrence of thrombotic complications between patients across various groups of cancer (p = 0.58). This is in contrast to other studies where there was a significant difference between occurrence of cardiovascular complication across types of cancer. The mechanism of synergy between COVID-19 infection and cancer leading to cardiovascular complication may be because of hyperinflammation, which negatively affects the cardiovascular system. The dysregulated immune response can promote cardiovascular and endothelial dysfunction manifesting as cardiovascular complication, but further studies are needed (Gupta et al. 2021).
The findings of this study revealed that the in-hospital mortality rate was among COVID-19 patients with cancer was 21.3%, with 208 out of 976 cancer patients succumbing to the illness. This mortality rate was lower than the estimate derived from a systematic review and meta-analysis of cohort studies involving hospitalized cancer patients with COVID-19, where the mortality rate was reported to be 30% (Desai et al. 2021). Another study conducted at Guy’s Cancer Centre and King’s College Hospital during the period from February 29 to July 31, 2020, reported a mortality rate similar to our cohort, at 24% (Sathishkumar et al. 2022). The in-hospital mortality among Solid and Haematological Cancer were (n = 72, 25%) & (n = 31, 21.09%) respectively. A cohort study of 2,515 adult cancer patients with COVID-19 published in JAMA found that haematological malignant neoplasms and lung cancer were associated with higher mortality rates, with an overall mortality rate of 38% (Várnai et al. 2022). Notably number of deaths were high in patients suffering from Genitourinary, gastrointestinal and lung cancers among solid cancers, non-Hodkin’s type of Lymphoma among Lymphomas, and Chronic lymphocytic leukaemia among Leukaemia’s, a pattern consistent with data previously reported from Tata Medical Centre in Kolkata, India, which also participated in the registry (Roy et al. 2021).
Adjusted hazard ratio models were employed to assess overall survival across various types of cancer compared to no reported morbidity, adjusting for age, gender, severity of disease at admission, cardiac complications, COVID-19 vaccination status, and commonly used COVID-19 treatments such as Remdesivir, steroids, and anticoagulants. Due to the non-proportionality of hazard ratios over time for different types of cancer, compared to those without comorbidities, adjustment for time interaction term for each type of cancer was also incorporated into the model. The model demonstrated that the risk of all-cause mortality for different types of cancer at day zero ranged from 531.8 to 25.74, with Non-Hodgkin’s Lymphoma and Head Neck brain Cancer malignancies exhibiting these extremes, respectively. Other cancers with significantly higher mortality are lungs and breast cancer. This is in line with previous studies that mention that lungs cancer has significantly high mortality when co-affected with COVID-19 (Lei et al. 2021).
The change in hazard ratio over time was also plotted, revealing that hazard ratios for all cancer types were significantly elevated immediately after admission but converged around and became similar to other comorbidities around days 10. This indicates that certain pathophysiology exclusive to cancer might play significant role in early mortality and hence should be dealt with aggressively. Also, this suggests that stringent facility-based management of cancer patients would be critical during this period. Additionally, the graph demonstrated that the time required for the hazard ratio to decline to one after hospitalization varied by cancer type: 17 days for genitourinary cancers, 13 days for gastrointestinal cancers, 11 days for lung cancer, 15 days for breast cancer, 18 days for head and neck cancers, 7 days for non-Hodgkin’s lymphoma, 15 days for chronic leukaemia, 14 days for acute leukaemia, and 13 days for unspecified cancers. Other comorbidities required 12 days. These findings indicate that extensive monitoring should be tailored considering the specific durations required for each cancer type following admission. Moreover, these results may be considered in the development of patient triaging protocols if needed during future hospitalizations.
The relatively high risk of mortality in the early days of hospitalization among cancer patients with COVID-19 may be attributed to their immunosuppressed state, which can make them more severely ill during the viremic phase, leading to more early deaths. Additionally, some reports suggest that receiving cancer treatment within 14 days of a COVID-19 diagnosis may pose a significant risk for developing severe complications. Many cancer patients, due to fear of contracting COVID-19, reported to hospitals only when necessary for cancer management. It may be possible that the relatively high mortality during the early days could be related to undergoing cancer treatment within 14 days of contracting COVID-19 (Cheng 2021; Sengar et al. 2022). The decreased risk of mortality observed in cancer patients beyond 14 days post-hospitalization may be attributed to surviving the initial viral load during the viremic phase and not experiencing immune-mediated complications, potentially due to their underlying immunosuppressed state (Bhaskar 2020). Above observation suggests that monitoring viral load at various time points, along with assessing the immune response, could be beneficial approach in optimizing treatment strategies for cancer patients. Further research is encouraged to validate these findings and refine clinical approaches.
In our investigation examining the impact of commonly used COVID-19 drugs, the addition of remdesivir and steroids to COVID-19 management regimen significantly reduced hazard of mortality as can be observed from reduction in Hazard Ratio in ICU patients. This finding contrasts with the Solidarity trial in terms of remdesivir, in which mortality was higher with remdesivir use among ventilated patients, although it was consistent with the findings of other studies (WHO Solidarity Trial Consortium 2022). The efficacy of remdesivir seemed to depend on various factors, including the need for oxygen or respiratory support and the timing of drug initiation, as evidenced by various trials. However, due to the lack of uniformity of available data for all patients, our data could not be further analysed in this regard. It is also worthwhile to mention here that Unadjusted hazard ratio associated with Remdesivir, indicates that the individuals who received the medication were at around 24% higher risk of dying as compared to those who did not. However, this result should not lead to the conclusion that the use of Remdesivir may have increased the chances of mortality because the administration of Remdesivir was not in random and, in practice, only individuals with severe infection or those at higher risk of severe outcome were prescribed Remdesivir. Also as discussed in previous studies age, male gender, severity of disease at admission, cardiac complication was significantly associated with higher risk of mortality within 30 days of hospital stay. While Covid-19 vaccination and commonly given COVID-19 drugs like remdesivir, steroids and anticoagulants reduce risk of mortality during hospital stay within 30 Days.
Additionally, cancer patients exhibited higher value of d-dimer with patients having solid cancer exhibiting higher median value, a biochemical proxy indicative of thrombotic complications and disease severity. This finding is similar with the outcomes of previous studies that reported elevated d-dimer levels among individuals with cancer (Ali et al. 2023). This observation contrast other studies that suggest patients with haematological cancers are at a higher risk of developing thrombotic complications when hospitalized with SARS-CoV-2 infection (Fernández-Cruz et al. 2022). Also in this study, we used the median CRP value of the cohort as a reference point (44.77 mg/L), and it was observed that patients with CRP levels exceeding 44.77 mg/dL were linked to an increased risk of overall mortality (model 2 Supplementary Table 1). This finding aligns with available data (Lentner et al. 2021; Rubio-Rivas, et al. 2022). Some studies have indicated that a CRP level of ≥ 40 mg/L is a good predictor of mortality. However, the optimal cutoff may vary depending on the methods and kits used in the assays. CRP has been acknowledged as a predictor of COVID-19 mortality in cancer patients (Lentner et al. 2021). Nevertheless, elevated CRP levels in cancer patients may be influenced by their underlying disease burden, suggesting that a higher cutoff may be necessary for predicting COVID-19 mortality in this cohort. Further research is needed to establish the optimal CRP cutoff for this population. A similar association was also noted with higher levels of d-dimer, value greater than 0.92,g/l (Ali et al. 2023).






Comments (0)