Enteroviruses are a large group of viruses that can cause serious health problems, such as meningitis in children [7]. Although they are most common in spring and summer, they can be isolated throughout the year. Typing EVs is important for studying the relationship between EV type and time of circulation and clinical syndrome, to find types or variants, and for epidemiological surveillance as the predominant enterovirus type varies from year to year [8,9,10].
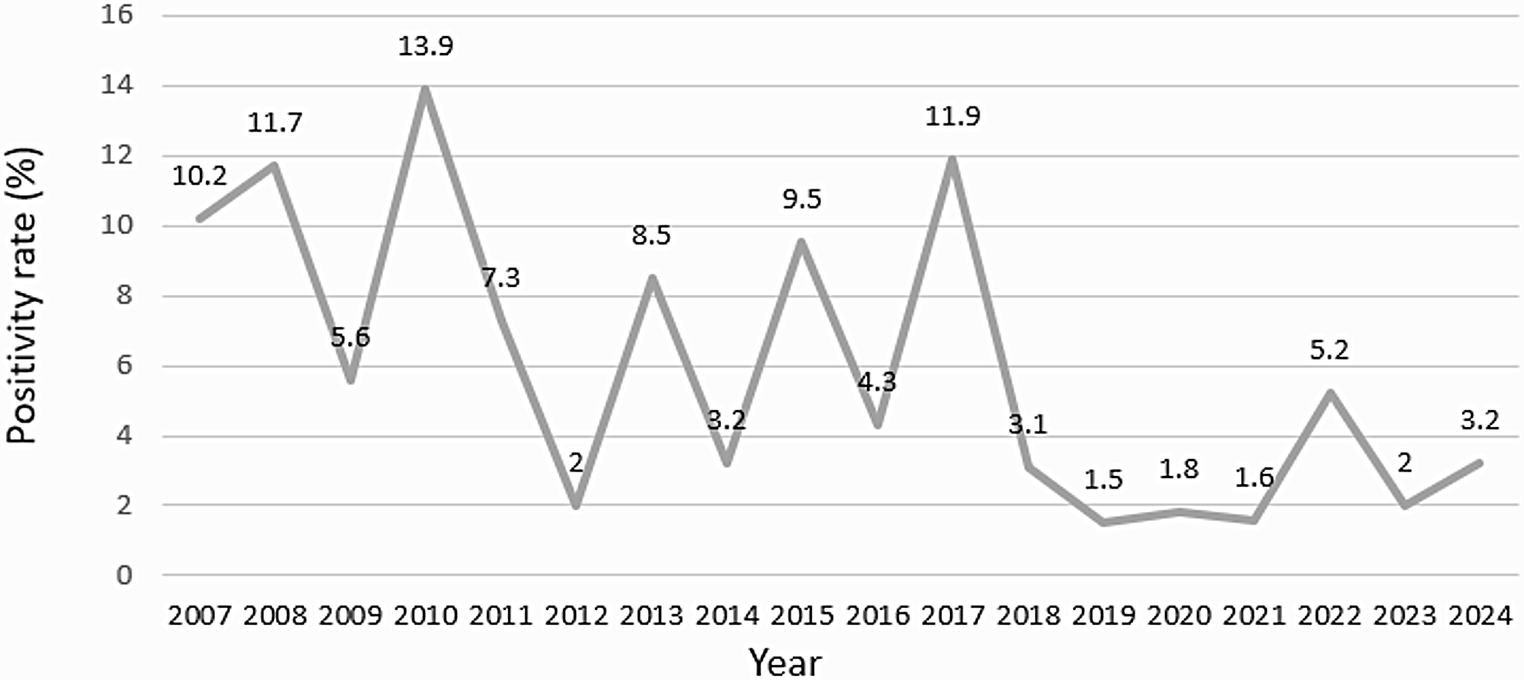
In a recent meta-analysis report, the median global prevalence was established at 6.3% [3]. In this study, the positivity rate was 5.7%, in the same range as previously reported, but differences were observed in different time periods. Before the pandemic, the positivity rate was around 9%. Interestingly, in 2019, just before the emergence of SARS-CoV-2, the positivity rate was halved (5.4%), although it should be noted that twice as many samples were examined as in previous years. In 2020, it fell to 1.27%. Subsequently, the next two years reached again 5.5%. In the last year studied, the positivity rate decreased to 2.57%, but it should again be noted the large number of samples studied. These data show once again that the measures taken during the pandemic had an impact not only on the circulation of SARS-CoV-2, but also on all other viruses and pathogens [10,11,12].
The age group with the highest positivity rate was, as expected, the youngest (10%) and decreased with increasing age (4.5% in children aged 6–14 years and 1.7% in adults) [7].
The most common species was A, followed by B, D and C, and it was associated to youngest children (under 6 years old). To characterise Enterovirus, 5’NTR has been used. Some reports recommend VP1 or other proteins as more specific, but in a recent report the species concordance between both fragments was 92% [14].
Generally, EV-A are mainly associated with herpangina and hand-foot-and-mouth disease (HFMD) and EV-B with herpangina and viral meningitis or encephalitis [15].A large study in Spain describing the epidemiology of EV infections from 2006 to 2020, identified 85% belonged to species A [16].This was expected as classically, the HFMD was associated with EV-A, principally CVA16 and EV-A71. Since 2009, the increased detection of CVA6 was already observed, displacing CVA16 as the main cause of HFMD. As in other neighboring countries, CVA6 emerged in Spain and is now considered an endemic serotype, being one of the five most frequent EV that circulate every year. In general, according to a recent meta-analysis by Brouwer et al., CVA6 is the most prevalent EV globally [3].CVA10 is another EV-A which began to be detected and associated with HFMD in the same period of time, both in Spain and in other countries. Although it is detected every year, it does so at low levels [16].
In our series, the predominant type in Asturias was CVA6 (32%) leaving CVA16 but less than 3%, and CVA10 did not get 1%. These data support the replacement of CV-A16, which during 2010 was the most frequently detected type in other studies, with CV-A6. And it was observed that CV-A6 was the unique EV found every year. CVA10 began to be detected in the last year, although this type, together with CV-A6, was one of the main causative agents of the outbreaks described during 2008–2010 in Finland, France and Spain [17]. Some publications describe the strong ability of CVA6 to produce HFMD in adults but in our sample only 3% were over the age of 15 [3].
On the other hand, while CV-A4 (12%) and CV-A2 (6%) were the most common and were found almost every year, CV-A8 was less frequently detected (1%), as in other studies [16, 18].
EVs species A was present in two out of three exanthematous disorders, but it was also associated with febrile syndromes and respiratory manifestations. It was less common in neurological syndromes.
In a recent meta-analysis cited above, EV-B types were the most common worldwide, with types CVA9, CVB1-5 and several echoviruses being particularly prevalent, and with echovirus 30 being the most common. They have been identified in children under one year of age and are characterized by severe disease with high mortality. In our sample, EV-B is only the second most common (35.6%) and was associated with children aged 6–14 years (63.6%), indicating small differences compared to the others [3, 16,17,18,19,20,21].
Although EV species B was also associated with respiratory manifestations and febrile syndromes, it was proportionally more common in neurological syndromes than other genotypes, representing the 64% of these cases.
The most common types were CVA9 and echoviruses E6, E7, E11 and E18, all among the most frequent. In Spain, E6 and E11 are among the ten most frequently reported [20].and EV13, considered rare in Spain and worldwide, was reported in 1% [21]. However, EV-30, long described as a cause of aseptic meningitis worldwide, is frequently detected in the Spanish territory, but was found in only 0,6% [19].
It is worth noting the difference observed before and after the SARS-CoV-2 pandemic. Before 2020, there were up to 13 types with higher positive rate, whereas after the pandemic only B5, E6 and E11 were found. It is likely that more types will be found over time.
CVA21 was the only EV type C reported in our sample and only 1case, EV-C were rarely found in studies conducted in Europe and were mostly found almost exclusively in stool samples [3].It should be noted that in this study 98% of the samples were from the respiratory tract.
Of the four EV-D types, EV-D68 is the only one found and represents a high positive rate. Analysis of EV-positive specimens collected from April 2014 to December 2018 from Spanish hospitalized patients with respiratory illnesses confirmed the presence of EV-D68 in almost half of the total characterized EV. It is known to cause predominantly respiratory disease, as it is noted in this study [3]. As previously reported, most of the EV-D68 infections were detected in young children. However, adult patients were also infected, half of them over the age of sixty [23, 24].In this study, EV-D68 was the fourth most common type found (10%) and thirty-eight% of patients were older than 14 years old. Furthermore, EV-D68 accounted more than half of the EVs found in this group. EV-D68 has also been associated with severe neurological cases, indicating the need for better surveillance of this EV [17].
As mentioned above, viral respiratory infections were strongly reduced during the most stringent public health measures to control SARS-CoV-2 transmission in 2020, but EVs re-emerged rapidly after they were relaxed [24].These measures adopted during the pandemic also reduced viral diversity. Up to 20 different types circulated before the pandemic, but only seven after.
This decrease in diversity was mainly observed in species B EV, as mentioned above.
On the opposite, CVA6 never disappeared and was the dominant type especially during the COVID epidemic (65%). The implementation of epidemic prevention measures did not eliminate the common type in Asturias. Given the serious and potentially life-threatening complications associated with hand-foot-and-mouth disease (in which CVA6 is widely implicated), the necessity of the prioritization of vaccine development is clear. Presently, inactivated vaccines demonstrate considerable efficacy, persistent immunogenicity and acceptable safety profiles within the vaccinated population [15].Our results suggest that only vaccines, including CV-A6, may be viable options for EV control in Asturias, and that the only approved EVA71 vaccines are irrelevant.
In 2022 situations returns to normality: prevention measures disappear and diversity will increase again. Types like A4, E11 and D68 reappear after easing the COVID-19 crisis isolation [25].
Factors that influence sequencing, such as viral load and sample quality, as well as the fact that PCR primers do not have the capacity to amplify all types, may explain the low number of sequenced samples. On the other hand, the sequenced fragment may not have sufficient resolution to identify a single type [26].
Due to the small sample size, the results may not accurately reflect the diversity or incidence circulating in this area, but given the importance of EV infection surveillance, it is a first insight and a stimulus for further studies where other regions of the virus can be studied to improve classification, and even attempt to study the whole genome by NGS methods, as was done in the SARS-CoV-2 pandemic.
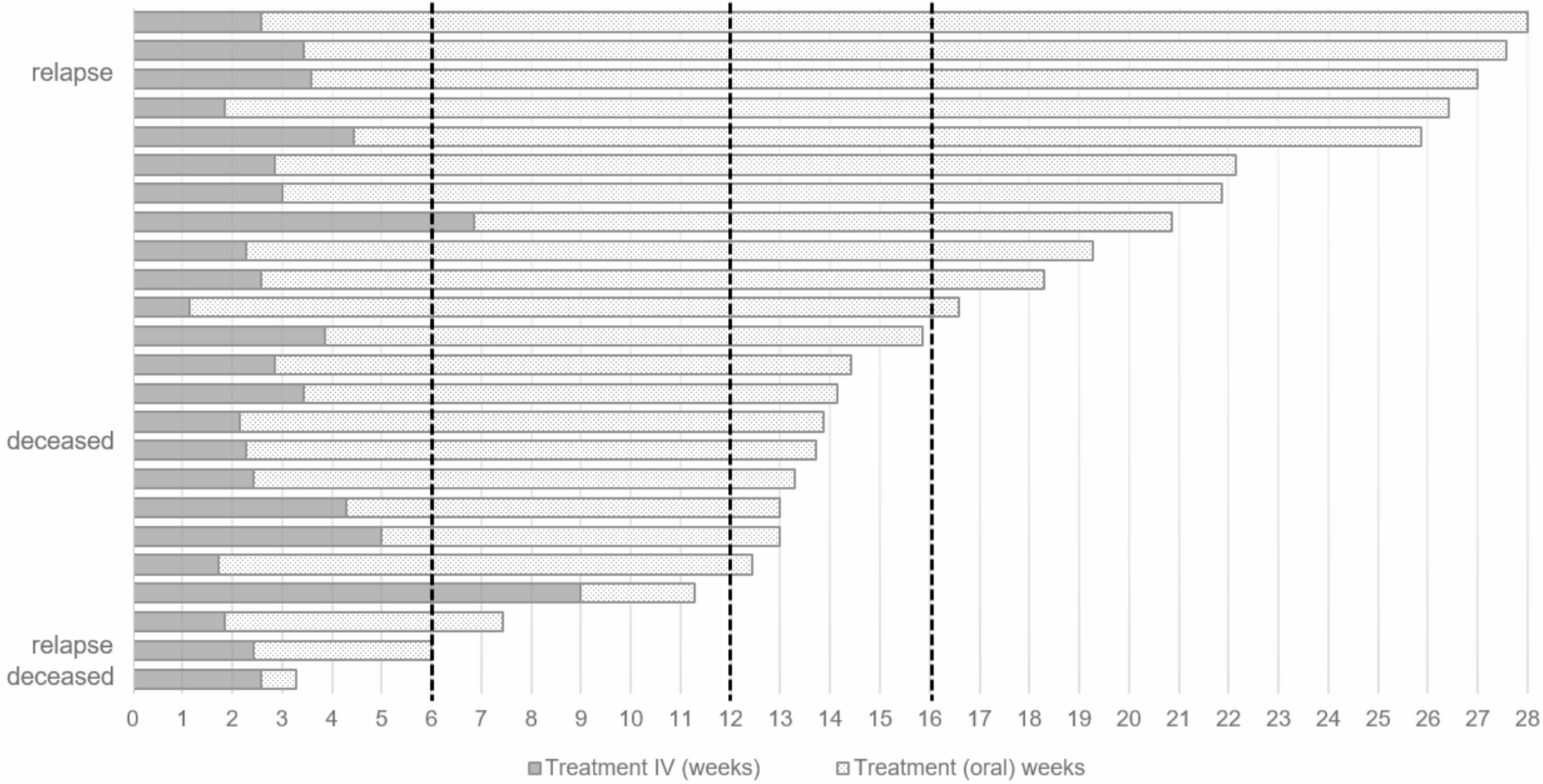
Finally, analysis of viral load in respiratory exudates, the most common specimen obtained for aetiological diagnosis, demonstrated the validity of the specimen and the high rate of viral replication in each clinical presentation. Moreover, this high replication rate is maintained at every site of EV infection, even in cerebrospinal fluid, where the mean viral load reached almost 5 log copies/ml.

Comments (0)