
Remember me
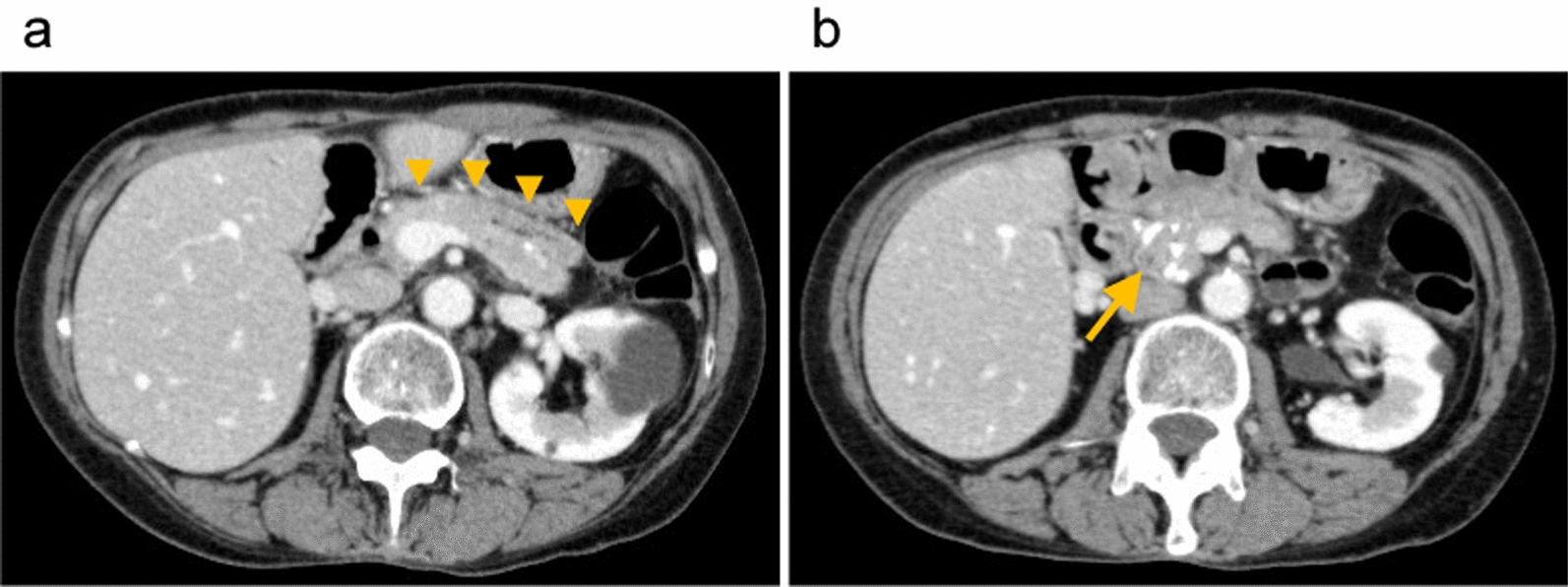




A 12-year-old girl was admitted to our hospital for left upper quadrant abdominal pain with an elevated fever. These symptoms continued for 7 days. The patient had no past medical histories except for a latex allergy. A physical examination revealed a fist-sized solid mass in the left costal region. The patient had spontaneous pain and tenderness on and around the mass. The patient’s vital signs were BT: 37.5 °C, BP: 92/62 mmHg, HR: 62/min, RR: 16/min. Except for slight anemia (Hb: 11.8 g/dL) and elevation of CRP level (5.98 mg/dL), her laboratory data was normal, and the levels of tumor makers were also within the normal range. Contrast-enhanced computed tomography (CT) revealed a well-circumscribed cystic and solid mass with hemorrhage measuring 8.3 × 5.3 × 7.1 cm in the pancreatic tail (Fig. 1a). The mass contained some calcifications in plain CT (Fig. 1b). T2-weighted magnetic resonance images (MRI) showed a nodular enhancement inside the mass suggesting a high cellular density lesion (Fig. 1c). According to the radiological findings, the mass was diagnosed as SPN of the pancreatic tail. It was difficult to trace the main splenic vein at the splenic hilum, but at the dorsal part of pancreas, the splenic vein was narrowed like as beak in enhanced CT images (Fig. 2a). This finding was considered that the splenic vein was compressed and stretched by the tumor. There was no splenic venous thrombosis or tumor invasion to the splenic vein.
Fig. 1
a Enhanced CT. An 8.3 × 5.3 × 7.1 cm cystic pancreatic tail tumor with hemorrhage (yellow arrow). b Plane CT. The pancreatic tail tumor partially contained calcifications (yellow arrow). c MRI T2-weighted image. A nodular enhancement inside the mass was suggested a high cellular density lesion (yellow arrow)
Fig. 2
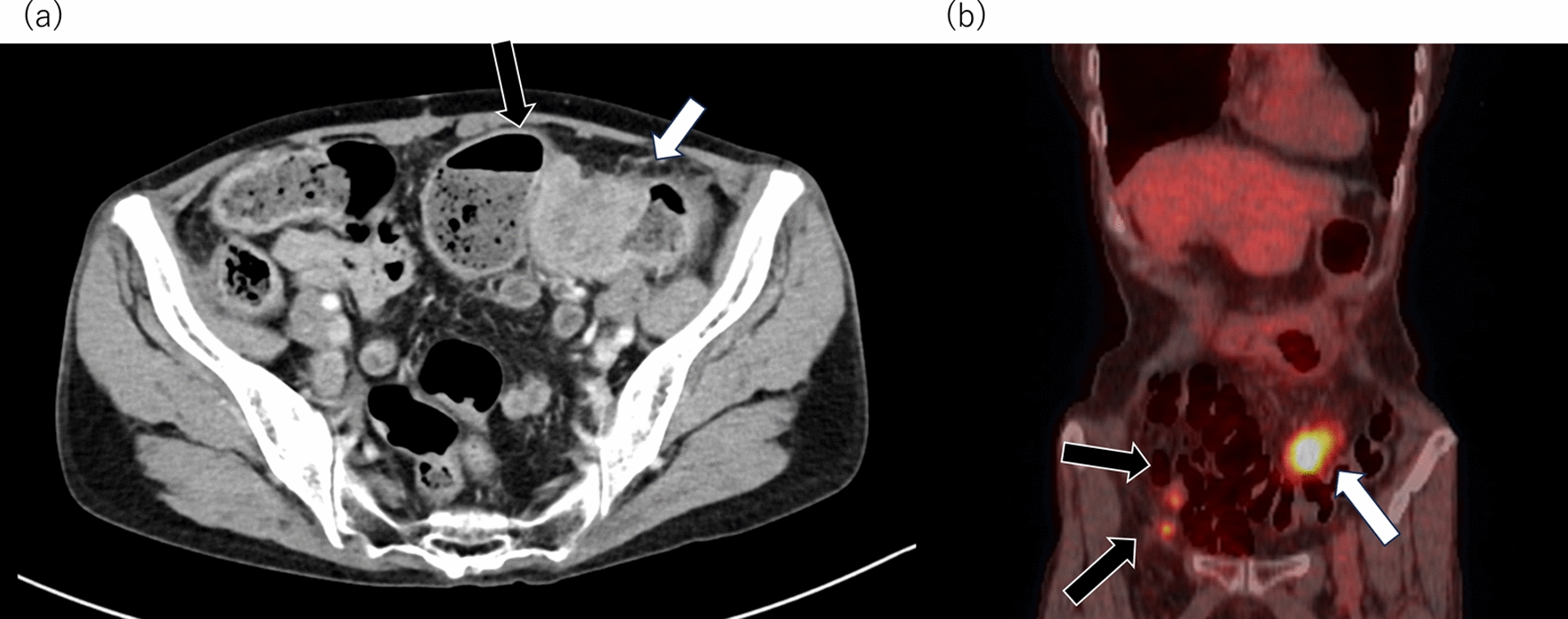
a Enhanced CT. a Shows that the splenic vein was narrowed like as beak due to compression and stretch by the tumor. b Enhanced CT. Collateral pathways developed through a short gastric vein and the left gastric vein (yellow arrow). Varices were developed in the gastric wall (red arrow). c Enhanced CT. A large spleno-renal shunt was developed (yellow arrow)
Abdominal ultrasound sonography (US) revealed that the spleen was enlarged (12.3 × 5.2 cm). Abdominal US and contrast-enhanced CT showed that multiple collateral pathways of short gastric veins and left gastric veins (Fig. 2b) with a large spleno-renal shunt had developed (Fig. 2c). These findings indicated left-sided portal hypertension (LSPH) due to tumor compression and stretch of splenic vein. LSPH and splenomegaly had already been observed at the time of diagnosis before the tumor resection. We discussed the possibility of spleen preservation at the time of surgery to prevent OPSI and decline LSPH after tumor resection. We concluded that splenic venous flow was resumed by tumor resection improving splenic vein stenosis caused by the tumor compression and stretch. Therefore, we chose the tumor resection with spleen preservation to prevent OPSI. We performed tumor enucleation by open surgery, the pancreas tail was partially resected due to severe adhesion. The stump of resected pancreas was closed by running suture. During the procedure, many dilated collateral splenic veins were seen. Some of the dilated collateral splenic veins were resected to detach the tumor.
Histological findings showed that the tumor consisted of solid lesions with pseudopapillary features and pseudo-rosette structures (Fig. 3a, b). Immuno-histochemical findings revealed that the tumor nuclei were positive in β-catenin (Fig. 3c). Based on those histological findings, the tumor was diagnosed SPN.
Fig. 3
a, b H&E. The tumor consisted of solid lesions with pseudopapillary lesions (yellow arrow). Pseudo-rosette structures were seen (yellow circle). c Immuno-histochemical findings. The tumor nuclei were positive in β-catenin staining
The patient was started enteral nutrition postoperative day (POD) 4, the drain discharges were 10–25 mL. The drain was clumped at POD 5. US showed no fluid retention around the pancreas tail, the drain was removed at POD 6. The patient had left lateral abdominal pain at POD 8 and the fluid retention around the pancreas tail was detected by US at POD 10. The patient did not show fever elevation. The laboratory data showed WBC: 3200, Amylase: 245 IU/L, Lipase: 203 IU/L, CRP: 3.07. Postoperative pancreatic fistula (POPF) was occurred. We started conservative treatment such as total parental nutrition and ulinastatin. Enhanced CT at POD 13 showed the splenic vein stenosis (Fig. 4a) and pancreatic tail cyst (Fig. 4b). The patient’s abdominal pain gradually improved and disappeared in 10 days without any infectious signs. The pancreas tail cyst was disappeared POD 29 by US without drainage. Moreover, a detailed anatomy of splenic vein and inferior mesenteric vein were revealed, the main tract of splenic vein did not detect but, the splenic venous flow at the dorsal part of pancreas was supplied through the pancreas parenchyma (Fig. 5). It suggested that the main tract of splenic vein was obstructed at the splenic hilum and the main tract of splenic flow did not improve after tumor resection. Although International Study Group of Pancreatic Surgery grade B POPF was occurred, the patient was discharged on POD 47.
Fig. 4
a Enhanced CT. Splenic vein stenosis remained at POD 13 (yellow arrow). b Enhanced CT. A cyst of POPF revealed at the stump of pancreas tail at POD 13 (yellow arrow)
Fig. 5
Abdominal US. A detailed anatomy of splenic vein and inferior mesenteric vein (red arrow) were revealed, the splenic venous flow (yellow arrow) at the dorsal part of pancreas was supplied through the pancreas parenchyma
The patient had no symptom, LSPH was remained after discharge by regular check-up. Six months after surgery, the patient developed a left quadrant abdominal pain that worsened during exercise. As a result, the patient could not attend school due to severe abdominal pain. Abdominal US showed that the splenic vein stenosis did not improve after tumor resection and LSPH with splenomegaly (spleen was measured by 12.7 × 47 cm) remained. Although laboratory data: (WBC 4200/μL, RBC 4.29 × 106/μL, and Plt 18.9 × 104/μL) showed that the hypersplenism was not seen in this patient, her abdominal pain was supposed to cause by splenomegaly induced by LSPH. Splenectomy was performed 9 months after the tumor resection. After the splenectomy, her abdominal pain disappeared and there has been no recurrence over the past 8 years. The patient received preoperative pneumococcal vaccination and postoperative prophylactic antibiotics for 2 years. In addition, the patient has continued to receive pneumococcal and meningococcal vaccination every 5-year post-splenectomy.
Comments (0)