
Remember me





A total of 100 pediatric patients, aged 1 to 3 years, undergoing below umbilical surgeries under general anaesthesia were included over a period of 2 months from April 2023 till June 2023, at two centres with 50 patients at each centres, after obtaining written informed parental consent. It was a prospective, randomized, observer-blinded clinical trial and was registered with trial registry number CTRI/2023/04/051251 dated 3/4/2023. Children with known blood coagulation disorders, systemic inflammation, inflammation in the area of the site of injection, and anatomical abnormalities of the lumbosacral spine were excluded from the study.
At each centre, 50 pediatric patients aged 1 to 3 years, undergoing below umbilical surgeries under general anaesthesia were included. They were randomly allocated with the help of computer generated random charts into two groups of 25 each to receive ultrasound guided local anaesthetic (LA) volume vs. Armitage formula based LA volume.
Prilocaine cream and an adhesive sterile tape was placed at the predetermined venous and caudal puncture sites and premedication was done with oral midazolam 0.5 mg/kg, 30 min before the procedure. The child was then transferred to the operation theatre and standard monitoring was applied (ECG, SpO2, non-invasive blood pressure). Incremental induction with 6 L fresh gas flow (FGF) and the sevoflurane dial set at 2% in a 2:1 mixture of N2O and O2 was done. The dial setting was increased by 1% every 2–3 breaths until loss of eyelash reflex, with a mean induction time of 1–2 min. After induction a peripheral venous access was established. Thereafter, sedation was supplemented with Inj. Fentanyl 2 ug/kg and I gel of appropriate size was then put and checked for the bilateral chest rise and by capnography. Spontaneous ventilation with sevoflurane (2%) in O2:N2O in a ratio of 33:66 was continued.
Ultrasound investigation, identification of T12 level, and conus medullarisThe child was then placed in the left lateral decubitus position with flexed lower limbs. We identified the 12th rib using linear 7–13 MHz ultrasound transducer (SonoSite Inc., Bothell, WA, USA) covered with transparent sterile adhesive and tracked it medially, thereby identifying the12th vertebral body and subsequently, the levels of the spinous process from T6 down to the conus medullaris were marked on the skin with skin marker. Subsequently, the probe was kept in transverse plane in the interspinous area, starting from level T12 till T4 and at each level the distance from ligamentum flavum to duramater was noted down.
Caudal block under ultrasound observationGroup UThe ultrasound probe was then kept over the sacral cornuae and the sacrococcygeal membrane was identified for the exact identification of the injection site. The sacrococcygeal membrane was punctured with a 24G short bevelled tip cannula confirmed by longitudinal probe orientation.
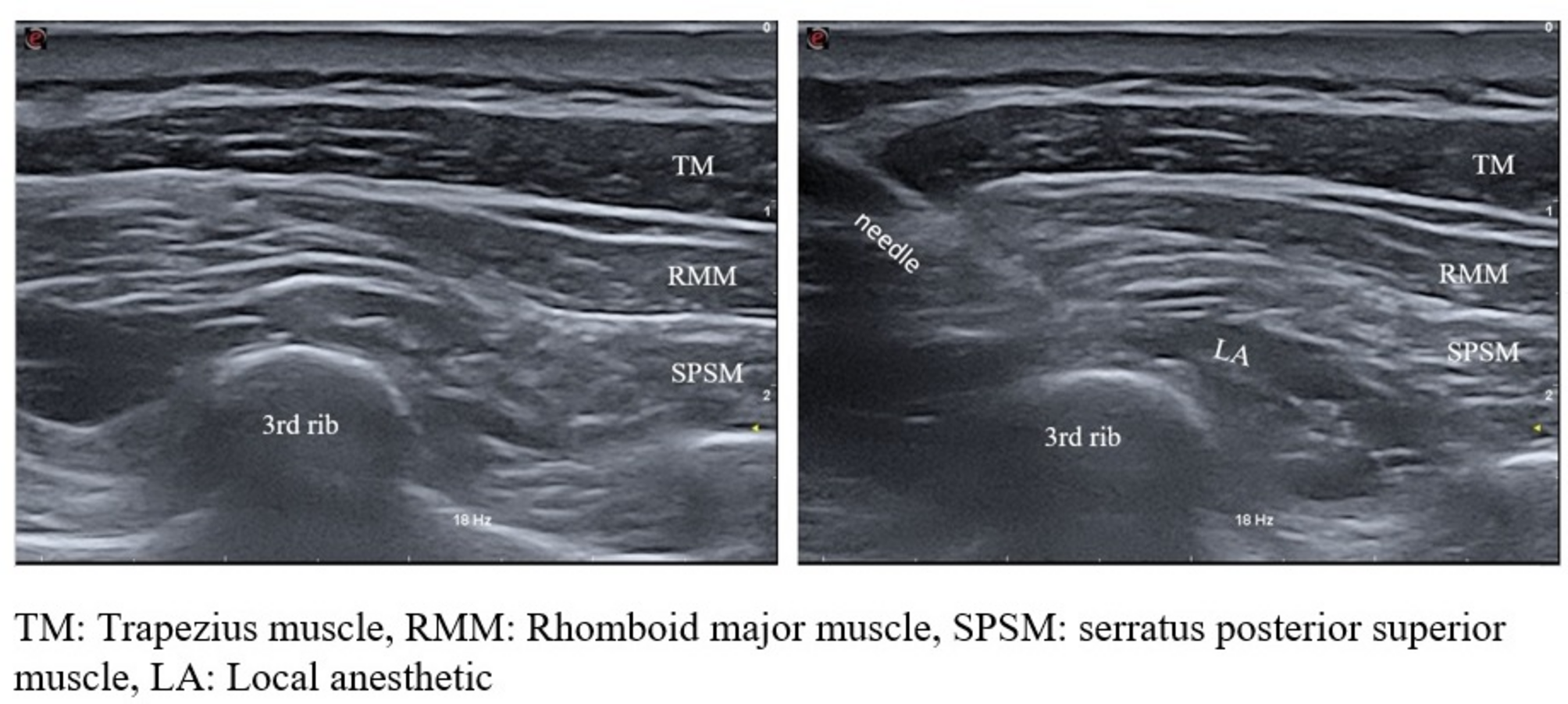
After that the ultrasound probe was kept in the median plane transversely at the level of T10 interspinous space and doppler mode was selected on ultrasound, to mark the color flow seen with advancement of drug on ultrasound [7]. After negative aspiration, 0.25% bupivacaine was injected at a speed of 0.5 ml/second and the drug injection was stopped immediately once the color flow in doppler was seen at T10 level. (Fig. 1) The drug volume was noted and dose of bupivacaine was calculated from the used drug volume in mg/kg. Because, even after stopping the drug, it still traverses into higher spaces so the same was noted by once again measuring the distance from ligamentum flavum to duramater from T12 to T4 interspaces, keeping probe in transverse plane and thus the maximum level reached was calculated by comparing the pre and post dilatation difference at each level. The highest level, where this difference was more than 20% was labelled as the maximally dilated highest space.
Fig. 1
Pre and post injection images of T10 epidural space visualizing the dominant color seen on doppler after the drug reaches T10 level
Group AThe drug volume was given as per Armitage formula that is 1 ml/kg of 0.25% bupivacaine for thoracolumbar region (T10) again at a 0.5 ml/second speed. The maximum level reached was also noted similarly as mentioned above.
One anesthetist was dedicated to perform the caudal block, including drawing-up and injecting the correct amount of local anesthetic, whereas a separate person was assigned to perform and evaluate the ultrasound scan. A second anaesthetist blinded to the drug volume injected performed the cutaneous testing at 15 min post-injection, to assess the highest dermatomal level of the block by observing flinching and facial expression in response to ice cube placed inside glove at different dermatomes.
Skin incision was performed 20 min after injection of the local anaesthetic. A successful block was defined as no motor (movements of extremities) or haemodynamic response (change in heart rate by more than 15%) to skin incision or during the surgical procedure, with no need for the administration of supplemental analgesics. In the case of a pain response (defined as: movements of the lower extremities, heart rate increase 15% from the baseline), children received analgesic supplementation as per institutional protocol in which case the block was considered a failure and the case was excluded from the study.
At the end of surgery I gel was removed after discontinuing inhaled anaesthetic agent and suctioning through I gel. Patients were observed in post anaesthesia care unit and then were sent to the ward after recording FLACC scores at 30 min post extubation as per institutional protocol [8]. The motor function of the lower extremities and the caudal puncture site was assessed in all children on the first postoperative day.
After 24 h, parental satisfaction scoring was assessed based on the NRS scale, that is score of 1,2,3,4,5 for totally satisfied, satisfied, moderately satisfied, somewhat satisfied and not at all satisfied respectively.
Statistical analysisThe data collected was recorded in MS Excel and analyzed viz. epinfo VT software. Qualitative variables were demonstrated as frequency and percentage. Quantitative variables were expressed as mean and standard deviation. Differences between both groups were studied by applying the Chi-square test and T-test according to study variables with P value < 0.05 was taken as statically significant. The sample size was calculated taking Confidence Interval of 95%, power of study 80% considering post operative pain at 30 min after shifting to PACU in Armitage group is 2.40 with SD of 0.58 and post operative pain at 30 min after shifting to PACU in ultrasound group is 1.08 with SD of 0.53 in previous study [9]. The final sample size came out to be as 60 (30 in each group) but to account for attrition and failures we took 50 in each group.
Comments (0)