
Remember me





Our discussion has eight subheadings. Those are; key facts of the case report, how did we conducted a systematic literature review to find similar reported cases, the relationship of the presented case with the existing literature, circumstantial evidence for and against suspecting heavy bupivacaine (ZUPIVAC H) as the cause of her seizures, explanation of the patient’s clinical and autopsy findings, differential diagnoses we considered at different stages, discussion of central nervous system toxicity by bupivacaine and possible mechanisms of toxicity and lessons to be learned and the way forward.
Key facts of the case reportAn ASA grade 2 pregnant mother underwent a routine a spinal anesthesia for a cesarean section and adequate anesthesia was achieved. After 5–7 min, she developed a progressive myoclonus that evolved into generalized tonic clonic seizures after delivery. Her seizures continued despite administering general anesthesia plus multiple anticonvulsants. She had rhabdomyolysis, one brief cardiac arrest, stress cardiomyopathy, central hyperthermia and died on day four. There were no significant radiological, macroscopic or histopathological changes in her brain or biochemical changes that explained her super refractory status epilepticus. Heavy bupivacaine samples from the same batch used for this patient were analyzed by two specialized laboratories. One laboratory reported that samples failed to confirm USP dextrose specifications. Bupivacaine samples passed all standard USP quality tests at the other laboratory. Nevertheless, they managed to detect an unidentified impurity in the medicine.
How did we conducted a systematic literature review to find similar reported casesSuper-refractory status epilepticus is rare and many doctors we know do not use that term. Thus, we decided to search for the word “status epilepticus” and select super-refractory status epilepticus cases out of those. We conducted a literature survey in several online databases in February 2024 for the keywords “status epilepticus”,“spinal anesthesia” and “case report” combined using the Boolean operator “AND”. Those databases were Google Scholar, PubMed, Europe PubMed Central, CNKI, ScienceDirect and DOAJ. A total of 576 articles were identified. Abstracts of each were read and 564 irrelevant articles were excluded. We used the PICO (P: patient/population/problem, I: intervention, C: comparison/control—O: outcome) framework to determine inclusion criteria [11]. Accordingly, we selected patients undergoing spinal anesthesia as our population, spinal anesthesia as intervention and super-refractory status epilepticus cases as the outcome. Out of the remaining 12, duplicates were removed, full articles were read and five cases that fulfill the definition of super-refractory status epilepticus attributed to a spinal anesthesia drug were identified. They were our references 2,3,5 and 6. The snowballing of those led to identification of our reference1. First and third authors independently did this process and obtained the same results.
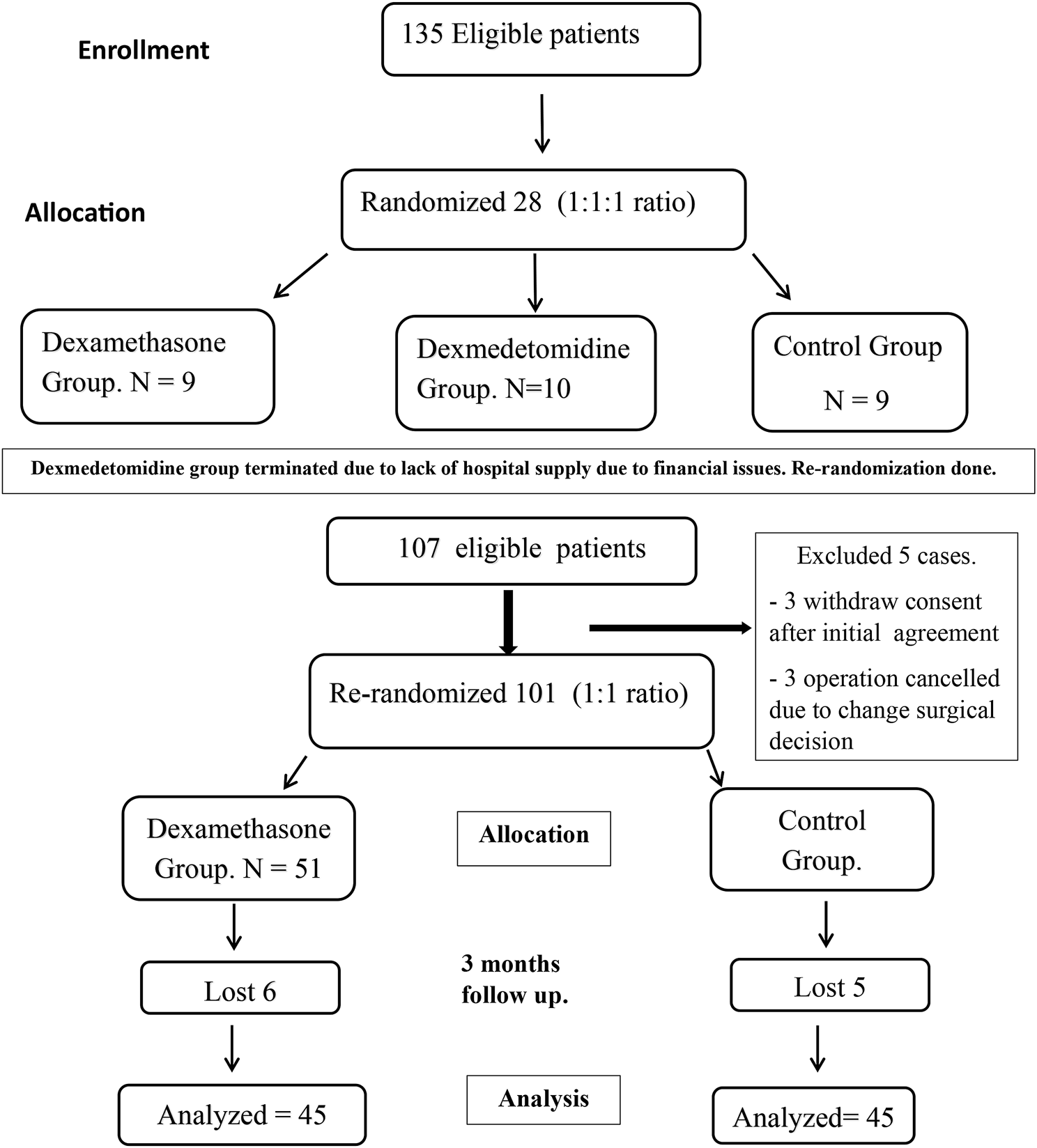
The flowchart of the process is shown in Fig. 1.
Fig. 1
The flowchart of systematic literature review process
In cases of reference1 and 6 the duration of seizures was not clearly mentioned, but their authors state that seizures continued despite the administering of anesthetic drugs. Super-refractory status epilepticus is primarily defined by failure to respond to appropriate treatment, not by seizure duration [12]. Hence, we included those two cases. The case of reference 7 has seizures for a few hours; hence we did not include that. Nonetheless, it is the first report (1994) of a status epilepticus (refractory status epilepticus) case following spinal anesthesia we found [7]. That patient had a history of seizures and tertracaine was used for anesthesia.
Earlier, we did a nonsystematic literature survey employing various strings. Among results for the string “local anesthetic systemic toxicity” AND “case reports” we have identified our reference 4. Key findings from past six reports of super-refractory status epilepticus attributable to spinal anesthesia are summarized in Table 1. The authors of some of those papers do not classify their cases as super-refractory status epilepticus cases.
Table 1 Key findings in past reports of super-refractory status epilepticus attributable to spinal anesthesiaRelationship of the presented case with the existing literatureSimilar to our case, all six cases were anesthetized using heavy bupivacaine. Only < 15 mg of bupivacaine was administered to all of them. However, sufentanil was added to heavy bupivacaine in two cases unlike us. None of them or our patient had any history of past seizures. Interestingly, 5/6 patients were women. Three past cases like our patient, had seizures minutes after spinal anesthesia while undergoing cesarean sections. One of them had a history of preeclampsia unlike our case. 3/6 had discomfort in the perineum or coccyx region before seizures and our patient complained of a discomfort that she could not describe. Like in our case, 3/6 had myoclonus or tremors prior to seizures. All past cases survived. None of the past cases had the combination of rhabdomyolysis, a brief cardiac arrest followed by stress cardiomyopathy and central hyperthermia.
There are several other reports of seizures associated with spinal anesthesia [3, 13,14,15]. Only two cases of seizures following spinal anesthesia was reported between 1945 and 1962 according to one author [13]. Reports have become more frequent lately (Table 1). A recent paper summarized 30 publications describing 31 patients and two cats who had had GTCS or myoclonus following spinal anesthesia [15]. Out of those cases, 64% resolved spontaneously and promptly and in 71% of cases neurotoxicity manifested 30 min after spinal anesthesia, in contrast to our case [15]. In the literature, there is a spectrum of cases varying from mild self-limiting myoclonus probably originating at the spinal cord level, to super-refractory status epilepticus cases like our case. We think the likely explanation for our case as follows. Initially, she would have had spinal myoclonus which was momentarily controlled by Midazolam. Although its density was higher than that of the CSF (as explained later), a minute fraction of administered ZUPIVAC H would have gradually reached the brain due to movement of cerebrospinal fluid and diffusion [16]. Then the drug acting on the brain would have initiated GTCS.
Circumstantial evidence for and against suspecting heavy bupivacaine (ZUPIVAC H) as the cause of her seizuresOur hospital uses about 400–450 ampoules of heavy bupivacaine per month at present. No similar incident happened at our hospital during the past 23 years to our knowledge. ZUPIVAC H brand arrived at our hospital for the first time, 45 days before this incident. Ampoules of batch No. DP2203 arrived at our hospital eight days before this incident. Another patient in our hospital developed refractory status epilepticus to ZUPIVAC H three days apart, arousing suspicion of something unique to ZUPIVAC H contributing to these events. Moreover, our patient had undergone spinal anesthesia with heavy bupivacaine (without adjuvants) five years before for her first LSCS, without complications. Therefore, we suspect that the impurity in the drug also contributed to her seizures. Nevertheless, there are reports of patients who had undergone uneventful spinal anesthesia, developing neurotoxicity during subsequent spinal anesthesia [15, 17]. Forty five patients in our hospital and more patients in other hospitals have undergone spinal anesthesia with ZUPIVAC H of the same batch without a problem on the same day and within the previous seven days. That fact is against suspecting a factor unique to ZUPIVAC H causing this event. Considering all this, we believe that ZUPIVAC H was the likely reason for her side effects and certain patient factors would have made our patient and the other patient of our hospital susceptible to the side effects of ZUPIVAC H.
Explanation of the patient’s clinical and autopsy findingsRapid onset of high fever, marked temperature fluctuations ending in death usually occur in central hyperthermia [18]. We think she had central hyperthermia owing to brain damage due to super-refractory status epilepticus plus possibly due to ZUPIVAC H [19,20,21]. Heat generated in muscles during seizures would have contributed to her fever initially, but when her temperature was highest (day 4) there were no seizures. High fever notwithstanding antipyretics and antibiotics, decline in CRP level from day 2 to day 4, normal CSF analysis results and negative central venous catheter blood and urine culture results indicate that infection is unlikely to be the cause of her hyperpyrexia. However, her neutrophil count was very high on day1 but gradually dropped. Her high neutrophil counts can be attributed to status epilepticus [20].
Neurocardiogenic pulmonary edema following status epilepticus is well documented [20, 21]. That explains her first day CXR changes. Our patient had a cardiac arrest on day 2 and resuscitated and on day 4 undergone a prolonged (> 1 h) cardiopulmonary resuscitation (CPR) before her death was confirmed. Respiratory tract infections (pneumonia) is the most common infection associated with status epilepticus [20].Those would have contributed to the changes in lungs observed at autopsy [20,21,22].
Rhabdomyolysis following status epilepticus is common and well known [20, 21]. Some drugs given to her like phenytoin and levetiracetam and pre-existing hypothyroidism may have aggravated rhabdomyolysis [23, 24].
Sudden unexpected cardiac arrest and death can happen in uncontrolled epilepsy [25]. Her cardiac arrest on day 2 may be attributable to status epilepticus [25]. The combination of effects of infused thiopentone and any bupivacaine cardiotoxicity also may have contributed to this. Although the echocardiogram did not depict characteristic left ventricular apical akinesia and ballooning, considering ST elevations in her ECG that appeared after doing the echocardiogram, very high troponin I levels and no blocks in coronaries observed at autopsy we think she may have had Takotsubo cardiomyopathy (stress cardiomyopathy) later. The stress of severe illness, first cardiac arrest and being on three inotropes also would have contributed to this. About 50 Takotsubo cardiomyopathy cases have been reported related to seizure activity, including 15 associated with status epilepticus [26]. Interestingly, there are reports of ischemic ECG changes, elevated troponin I with normal coronary angiography without seizures resulting after spinal anesthesia described as bupivacaine induced cardiac toxicity by reporting authors [27, 28].
Histopathological changes in her kidneys and liver are likely to be due to hypoxemia during prolonged resuscitation after the second cardiac arrest. Liver dysfunctions occur in 25% of patients with rhabdomyolysis by various mechanisms including the released proteases causing liver inflammation [29]. This explains her high liver enzyme levels. Drugs like levetiracetam also might have contributed to kidney injury [30]. Her proteinuria is likely to be due to myoglobinuria.
A CSF analysis depicting chemical meningitis was reported in a past patient who had seizures following spinal anesthesia [31]. Nevertheless, our case and some similar cases did not show CSF evidence of chemical meningitis [1,2,3, 5].
As explained above, her rhabdomyolysis, central hyperthermia, cardiomyopathy and postmortem changes observed in her lungs, kidneys and liver may be largely due to her super refractory status epilepticus with contributions from other factors. Her status epilepticus was due to ZUPIVAC H. That initiated the train of events leading directly to her death. Hence, the side effect of ZUPIVAC H most probably was her underlying cause of death [32]. However, we do not have adequate information to specifically identify the responsible component(s) of ZUPIVAC H.
Differential diagnoses we considered at different stagesWe initially suspected a high spinal or local anesthetic systemic toxicity (LAST). In a patient with short stature and obesity, a high spinal can occur with a regular dose of heavy bupivacaine. The presence of a clear sensory level with preserved handgrip, the absence of any bloody tap, administering only 12.5 mg of bupivacaine, absence of other symptoms of LAST and no initial cardiac involvement indicated that those two possibilities are unlikely. At the end of the day1 and thereafter an adverse reaction to ZUPIVAC H, amniotic fluid embolism, normotensive eclampsia and previously undiagnosed brain pathology were the differential diagnoses. Amniotic fluid embolism is unlikely as at the onset there was no hypoxia with severe respiratory symptoms or cardiovascular collapse. Myoclonus is not the first sign of amniotic fluid embolism. Laboratory tests did not show significant coagulopathy. Later histopathology of the lungs also did not show evidence of amniotic fluid embolism [33]. Normotensive eclampsia is unlikely because there were no prior proteinuria, excess edema, or prodromal symptoms and onset of super-refractory status epilepticus after the delivery that did not respond to vigorous treatment [34]. Normal NCCT brain and later autopsy findings excluded previously undiagnosed brain pathology. Malignant hyperthermia (in addition to seizures) after giving suxamethonium is another possibility. However, reduction of ETCO2 to 34-40mmHg range after admission to the ICU, fever spikes appearing on the following day (after the decrease of ETCO2) and peaking on day 4 were against this possibility. Meningoencephalitis (infection) was also suspected as a reason for the high fever. The CSF analysis and autopsy findings excluded that possibility. At the end of both institutional death reviews, the final consensus was that this was an idiosyncratic reaction to ZUPIVAC H. After the extensive literature review by the first author, considering all available information, we now believe that this is most probably a case of direct local on-target type (mechanism-based) neurotoxicity on the CNS. As explained later, this can be categorized as an idiosyncratic reaction to ZUPIVAC H as well.
Discussion of central nervous system toxicity by bupivacaine and possible mechanisms of toxicityThe International Union of Basic and Clinical Pharmacology (IUPHAR) defines an adverse drug reaction (ADR) as an unwanted or harmful reaction experienced following the administration of a drug or combination of drugs under normal conditions of use and is suspected to be related to the drug [35]. Accordingly, this is an ADR. IUPHAR defines a side-effect as any effect caused by a drug other than the intended therapeutic effect [35]. The cesarean section was performed up to the delivery of the baby under spinal anesthesia induced by this drug alone (therapeutic effect was there). Additionally, there was this fatal side effect [35]. The United States Food and Drug Administration (FDA) use the terms adverse reactions and side effects as synonyms [36]. The IUPHAR defines drug toxicity as adverse effects of a drug that occur because the dose or plasma concentration has risen above the therapeutic range, either unintentionally or intentionally [35]. Accordingly, this is very unlikely to be drug toxicity due to the following reasons. She was given a therapeutic dose that has been in use worldwide for a long time [37]. Spinal anesthesia was working well during the onset of the seizures indicating that a certain percentage of drug molecules were bound to spinal cord receptors. Normally, the peak plasma concentration increase is approximately 0.4 mg/l (0.4 µg/ml) for every 100 mg of bupivacaine injected intrathecally and that peak takes about 50 min to occur [38]. Considering that there was no bloody tap, the maximum plasma concentration that possibly would have been achieved in 10–15 min after injection was very much lower than 2–3 µg/ml toxic threshold [38, 39]. Some authors of past similar case reports considered their cases as LAST [3, 4]. Nevertheless, LAST is a term to be used if plasma concentration exceeds the therapeutic range [4, 39,40,41,42]. Anesthesiology trainees in Sri Lanka and elsewhere learn > 2 mg/kg as the toxic dose of bupivacaine unless it accidentally gets injected intravascularly [40, 42]. Our patient was administered a far lower dose. Hence, LAST may not be an appropriate categorization for cases like this. Local neurotoxicity by local anesthetics is mentioned by a few past authors [41, 43]. We think our case and similar cases following spinal anesthesia are more likely to be due to a category of direct local on-target type (mechanism-based) neurotoxicity on the CNS [44]. This category of toxicity appears to be occurring at unexpectedly low plasma and CSF concentrations, happens very rarely, thus, patient factors may also be playing a role. A case of cardiac toxicity (without seizures) following only 1.1 mg/kg of bupivacaine, injected cutaneously, was reported in a l-carnitine deficient patient [45]. This is one example of patient factors increasing the risk of bupivacaine toxicity. An experiment demonstrated that administration of supplemental l-carnitine could reverse this risk in rats [46]. Interestingly, l-carnitine deficiency is associated with seizures, cardiomyopathy, rhabdomyolysis, etc. as well [47, 48]. We could not screen her for l-carnitine deficiency.
Toxic reactions usually occurs when the plasma concentration of total (bound and unbound) bupivacaine rise ≥ 2–3 µg/ml (generally ≥ 4 µg/ml) and when the unbound concentration ≥ 0.1–0.2 µg/ml [41, 50]. Nonetheless, there is a report of an experiment where a similar aged healthy woman was slowly intravenously infused with bupivacaine and developed GTCS at a plasma concentration of ≥ 1.1 µg/ml [49]. Cases like ours may have been liable to develop seizures at even lower thresholds due to unidentified factors peculiar to the patient.
Further investigations into future similar cases, for patient factors like l-carnitine and alpha-1-acid glycoprotein deficiency (bupivacaine mostly binds to this protein) etc. would be helpful to clarify the pathophysiology of such events.
Another possible patient factor was either abnormal function or concentration of cell membrane receptors or both. We give an example. In one study, GIRK:Kir3 potassium channels of cell membranes were inhibited within seconds of bupivacaine application [50]. Other voltage-gated potassium channels are also inhibited by bupivacaine [50]. Those channels inhibition increase membrane excitability, which can result in seizures [50]. In one experiment, mice were genetically modified resulting in a lack of similar GIRK2 receptors [51]. They had spontaneous seizures and were prone to pharmacologically induced seizures as well [51]. Had her brain GIRK:Kir3 receptors been sparse, inhibition of existing ones by bupivacaine would have contributed to her seizures [50]. We do not have facilities for further investigation in that line. The impurity appeared to be structurally related to bupivacaine. Thus, it is reasonable to speculate that the impurity might also have inhibited those receptors, perhaps even stronger than bupivacaine. Further studies are necessary to clarify this matter.
Bupivacaine (regular) used for spinal anesthesia comes as a racemic mixture. Had bupivacaine administered to this patient contained more R-(+)-enantiomer, which is more potent that could have been more toxic at a lower dose [52, 53]. We could not test ZUPIVAC H for enantiomers.
95% of bupivacaine in plasma is protein bound [40]. Bupivacaine binds to alpha-1-acid glycoprotein and to a lesser extent to albumin in plasma and in the CSF and unbound bupivacaine is responsible toxic effects [
Comments (0)