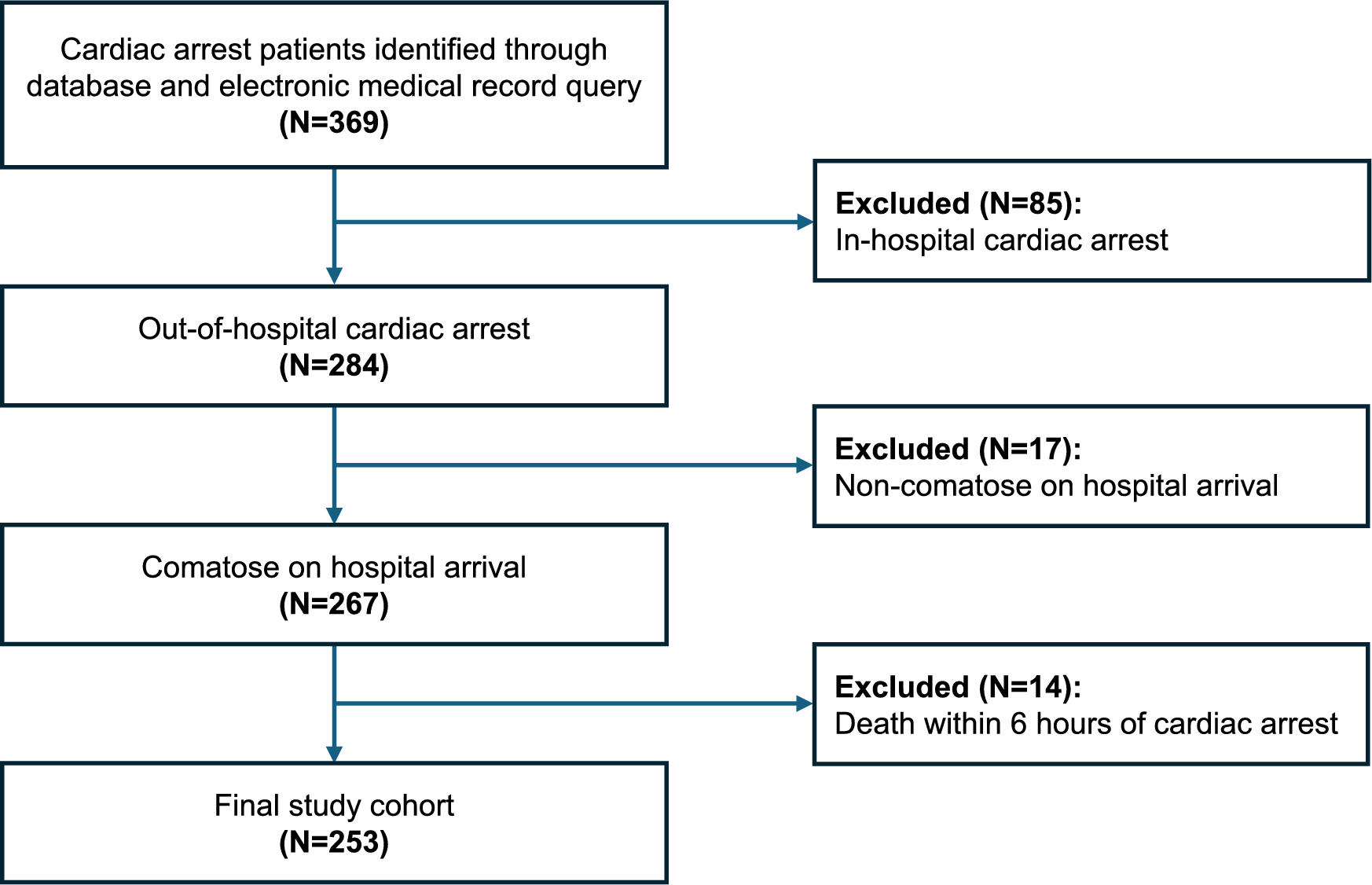
This is a retrospective analysis of data collected in an ongoing prospective observational cohort study on consecutive patients with spontaneous SAH and cerebral microdialysis admitted to the neurological intensive care unit of a tertiary referral center between 2010 and 2016. The article was written according to the Strengthening the Reporting of Observational studies in Epidemiology guidelines. All provisions of the Helsinki Declaration were followed. The conduct of this study was approved by the ethics committee of the Medical University of Innsbruck, Austria (AN3898 285/4.8), and informed consent was obtained from all patients or a legal representative, according to Austrian legislation. Inclusion criteria were age above 18 years, the admission diagnosis of spontaneous SAH, and cerebral microdialysis monitoring for at least 48 h.
Treatment and Grading
The treatment of patients conformed to current international guidelines, with the exception of nimodipine being administered intravenously [10, 11]. Ruptured aneurysms were treated early, either by endovascular coiling or neurosurgical clipping. If no aneurysm was detected, a repeat conventional angiography was performed 2 weeks after admission. All patients were mechanically ventilated during the period of invasive neuromonitoring and routinely received continuous midazolam and sufentanil. In case of hydrocephalus, an external ventricular drain was placed. If intracranial hypertension (> 20 mm Hg for > 5 min) was detected, despite routinely performed preventive measures (head and upper body positioning, adequate sedation, normoventilation, normothermia), possible interventions included deeper sedation, mild hyperventilation, osmotherapy, and, in refractory cases, hemicraniectomy. All patients were monitored by transcranial color-coded duplex sonography. When severe vasospasm (> 200 cm/s) was detected, induced hypertension with a target cerebral perfusion pressure (CPP) > 80 mm Hg was applied, and intraarterial nimodipine administration was considered. DCI was defined as a new infarct detected by cerebral computed tomography (CT) or magnetic resonance imaging scanning, not attributable to other causes [12]. Functional outcome was prospectively assessed 3 months after intensive care unit admission by a telephone interview, performed by a trained study nurse masked to clinical data, using the modified Rankin Scale. Scores of 0–2 were defined as favorable outcomes, and scores of 3–6 were defined as unfavorable functional outcomes.
Clinical disease severity was graded using the Hunt and Hess scale. Cerebral CT was performed on admission, after aneurysm treatment, and whenever clinically indicated. The initial CT scans were graded by a neuroradiologist using the modified Fisher score and screened for the presence of global cerebral edema [13, 14]. Microdialysis probe location was defined as “perilesional” if the gold tip of the probe was within 1 cm of a focal CT hyperdense or hypodense lesion or, if not, as “normal-appearing brain tissue” [15].
Cerebral Microdialysis
Invasive neuromonitoring, including cerebral microdialysis, was performed in patients who were expected to be mechanically ventilated for more than 48 h and showed clinical and/or radiologic signs indicative of raised intracranial pressure as part of clinical routine monitoring. CMD catheters (71 High Cut-Off Brain Microdialysis Catheter; M Dialysis AB, Stockholm, Sweden) were tunneled and placed into the white matter of the brain region deemed to be at the highest risk of developing secondary brain injury (the vascular territory of the ruptured aneurysm or the region exhibiting the severest focal brain lesion). Isotonic perfusion fluid (Perfusion Fluid CNS; M Dialysis AB) was pumped through the microdialysis system at a flow rate of 0.3 µl/min. Hourly samples were immediately analyzed with a CMA 600 or Iscusflex (M Dialysis AB) for CMD-glucose, CMD-pyruvate, CMD-lactate, and CMD-glutamate concentrations. At least 1 h passed between the insertion of the probe and the start of sampling. Neuroglucopenia was defined as CMD-glucose < 0.7 mmol/l, metabolic distress was defined as lactate-to-pyruvate ratio (LPR) > 40 and mitochondrial dysfunction as LPR > 30 together with pyruvate > 70 µmol/l [3].
Glycemic Control and Liberalization
Our institutional protocol aims at maintaining serum glucose concentrations between 110 and 180 mg/dl (6.1–10 mmol/l). Continuous short-acting intravenous insulin is administered if serum glucose concentrations exceed this threshold. Within this range, the determination of a patient’s individual serum glucose target is left to the discretion of the treating physician, also considering CMD-glucose levels. To investigate the impact of systemic glucose on brain glucose levels, we defined a liberalization event as a day with a median serum glucose concentration < 150 mg/dl (8.3 mmol/l) followed by a day with a median serum glucose concentration > 150 mg/dl (8.3 mmol/l) and compared variables (especially the frequency of neuroglucopenia) between these consecutive days. This way, we sought to investigate the impact of changes of serum glucose levels from the “lower normal range” (i.e., 110–150 mg/dl) to the “higher normal range” (150–180 mg/dl) on cerebral physiology within individuals on directly consecutive time frames. Hyperglycemia was defined as serum glucose > 200 mg/dl.
Statistics
Numeric data are shown as counts and percentages per group. Continuous data were assessed for normality using the Shapiro–Wilk test and are shown as means and 95% confidence intervals or as medians and interquartile ranges. Repeated measurements within study participants were performed using generalized estimating equations, choosing the regression matrix with the best fit for the data. Cases with missing values were included. For the assessment of temporal dynamics, “day after the hemorrhage” was inserted as a factor in a linear model, with CMD-glucose (single values) or percentage of daily neuroglucopenia (percentage of measurements per day per patient) as an outcome variable. In a similar manner, the impact of liberalization was analyzed by inserting the binominal “before and after liberalization” variable as factor into a linear model. The impact of CMD-glucose on functional outcome was assessed in a binary-logistic model, with the dichotomized modified Rankin Scale as an outcome variable and CMD-glucose (single values) or percentage of neuroglucopenia (percent of measurements per day per patient) as a covariate. The level of significance was set at a p value < 0.05. All analyses were performed with SPSS (Version 24.0; IBM SPSS Statistics, Armonk, NY).





Comments (0)