
Remember me

In the present issue of the Journal Block and collogues report the intriguing results of the 36 month follow-up of the RADIANCE-HTN TRIO Trial, a study investigating the efficacy and safety of the renal denervation procedure based on endovascular ultrasounds in the hypertensive state resistant to antihypertensive drug combination treatment [1]. The study enrolled patients with true resistant hypertension, defined accordingly to the indications included in the most recent guidelines on hypertension diagnosis and treatment issued by the European Society of Hypertension (ESH) [2], and under a 3-drug pill combination treatment [2]. A sham control group not underwent ultrasound renal denervation was taken as comparator. Results provide clearcut evidence that the procedure maintains its blood pressure lowering effects throughout the long-term follow-up period, the average clinic systodiastolic blood pressure reduction after 36 month observation being superimposable for magnitude to the one recorded few weeks after the procedure (−8.0 ± 24.5/−5.0 ± 14.6 mmHg vs −9.3 ± 18.1/−4.7 ± 12.1 mmHg, mean changes±standard deviation, P = NS) [1, 3].
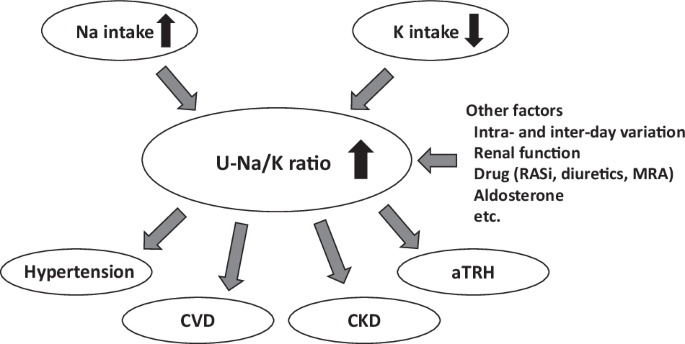
The intriguing long-term results of the trial offer the chance to make some considerations on the pathophysiological and clinical relevance of the ultrasound-based renal denervation approach in drug-resistant hypertension. The first consideration refers to the analysis of the efficacy of the endovascular ultrasound approach compared to other renal denervation procedures adopted in previous studies. As shown in Fig. 1, the blood pressure reduction, detected after few weeks from the procedure, was quite similar for magnitude in the different sham-controlled clinical trials of second generation performed with various methodological approaches to obtain renal denervation [4]. In addition, the clinic blood pressure lowering effects of the renal denervation procedure based on endovascular ultrasounds appear to be significantly more marked for systolic than for diastolic blood pressure, a finding which has been also confirmed by the analysis of the data collected at the 36 month follow-up.
Fig. 1
Effect of renal denervation in different published clinical trials (indicate by the acronyms). Bar graphs represent the change in office blood pressure after different renal denervation (RDN) procedures observed in the sham-controlled randomized clinical trial of second generation. Data are shown as systolic (SBP) and diastolic (DBP) blood pressure changes from baseline to the time point of each study primary objective. P values are given for difference between treatment and sham group adjusted for baseline blood pressure
A second consideration refers to the fact that the present report [1] does not provide any information on 24-h ambulatory blood pressure values, at variance from the original paper based on data collected few weeks after the procedure [3]. This appears to be an important limitation, considering the major advantages of ambulatory blood pressure compared to clinic blood pressure in the assessment of the clinical profile of the hypertensive patients. According to recent ESH guidelines [2] these advantages include: 1) a greater reproducibility of 24-h mean blood pressure values compared to the office ones, 2) a closer prediction of target organ damage, 3) a better prediction of outcomes and mortality, 4) the possibility to discriminate between apparent and true resistant hypertension, 5) the ability to identify white-coat and masked hypertension and 6) the quantification of the main 24-h blood pressure features, such as blood pressure variability, morning blood pressure surge and dipping status, i.e. all conditions which may have an important impact on patient’s prognostic profile [2, 5, 6]. Altogether these peculiar properties make a superior ability of 24-h ambulatory blood pressure data, compared to clinic blood pressure values, to stratify in a given study population the total cardiovascular risk.
Two further comments on the RADIANCE HTN follow-up study deserve to be made. The first one refers to the mechanisms which may be responsible for the blood pressure lowering effects of the renal denervation procedure based on endovascular utrasounds. Similarly to the hypotheses advanced throughout the years for explaining the blood pressure reduction documented following radiofrequency renal nerves ablation, it can be suggested that the blood pressure lowering effects of the procedure might depend on metabolic factors, such as for example an improvement in tissue insulin sensitivity leading to e a reduction iin insulin resistance [2, 7]. They might also depend, however, on the effects of the procedure on the renin-angiotensin system, leading to a reduction in the circulating plasma levels of anngiotensin II, a neurohumoral substance with well defined systemic vasoconstrictor and pressor effects [2, 7]. A more likely hpothesis identifies in the sympathoinhibitory effects associated with the renal denervation procedure, independently on the methodological approach used to achieve a full bilateral denervation of the renal nerves, the main mechanism repsonsible for the blood pressure lowering effects [2, 8]. The information so far available on this issue are scanty, particularly when the results of the endovascular ultrasound approach are examined. It should be mentioned that in the case of the radiofrequency ablation of the renal nerves our group has shown that the procedure exerts a marked reduction in sympathetic nerve traffic dIrectly quantified via the microneurographic technique [9]. However, no quantitative relationship was detectable in our resistant hypertensive patients between the blood pressure and the sympathetic responses to the denervation procedure iobserved during the 6 month follow-up. In addition we found a marked variability of the sympathetic and the blood pressure responses, with the possibility to detect blood pressure reduction in patients in which sympathetic nerve traffic was virtually unchanged. This allowed us to conclude that in the case of radiofrequency renal denervation the blood pressure reduction appears to occur independently of the sympathetic deactivation triggered by the procedure. Wheter this is the case for the endovascular ultarsound approach for renal denervation remains to be seen.
Finally, the report of the long-term results of the RADIANCE-HTN Trio trial does not include information about the heart rate responses to the procedure in the study population during the follow-up. Given the evidence that heart rate may represent a quite sensitive, although indirect, marker of the sympathetic cardiovascular drive [10], this information should allow to provide some insights on whether and how sympathetic activity is affected by the procedure, concurring at determining its blood pressure lowering effects.
In summary, despite the above limitations, the paper by Block and collegues [1] has an undisputed merit, namely the documentation on the efficacy and safety of endovascular ultrasound as a procedure capable to effectively lower clinic blood pressure values during the long-term period in true resistant hypertensive patients.
Comments (0)