
Remember me




Myocardial infarction (MI) is a common cardiovascular disease with high disability and mortality rates, and its incidence is increasing annually. Ventricular arrhythmias, such as ventricular tachycardia and ventricular fibrillation, are the main causes of cardiac arrest after MI and seriously threaten the lives of patients. Therefore, it is important to decrease the occurrence of ventricular arrhythmias after MI. Sympathetic remodeling and activity are closely related to ventricular arrhythmias after MI.1–3 Previous studies have shown that sympathetic remodeling, which is a change in the distribution and density of sympathetic nerves, occurs after MI. The NGF/TrkA pathway plays a critical role in sympathetic remodeling.4 Nerve growth factor (NGF) is required for the survival of sympathetic neurons and promotes their growth and survival via activation of tyrosine kinase receptor A (TrkA).5,6
Sodium-glucose cotransporter 2 inhibitors (SGLT2is) are a class of hypoglycemic drugs that include empagliflozin (EMPA), dapagliflozin (DAPA), canagliflozin, sotagliflozin, and ertugliflozin. They reduce the renal threshold for glucose and increase its excretion in urine by inhibiting the active glucose reabsorption by SGLT2 of the proximal renal tubules, thus lowering blood glucose safely and effectively.7 They also significantly reduce the occurrence and progression of heart failure and cardiovascular events.8–12 Compared with angiotensin receptor-neprilysin inhibitor (ARNI) monotherapy, ARNI combined with SGLT2is therapy could reduce hospitalization and mortality in patients with heart failure with preserved ejection fraction (HFpEF).13 In patients with HFrEF, compared with omecamtiv mecarbil and vericiguat, SGLT2is can significantly reduce the risk of heart failure hospitalization, and were superior to omecamtiv mecarbil for cardiovascular death and all-cause death.14 In recent years, an increasing number of experiments have demonstrated that SGLT2i can significantly reduce the occurrence and development of arrhythmias. Results of the DECLARE TIMI 58 trial showed that DAPA reduced the risk of atrial fibrillation/atrial flutter by 19% in the patients with type 2 diabetes.15 Azam et al.16 confirmed that EMPA can reduce the induction rate of ventricular fibrillation after MI.
The present study investigated the effects of EMPA on ventricular arrhythmia amelioration by inhibiting sympathetic remodeling and sympathetic activity after MI.
Methods Establishment of the animal modelSixty male nondiabetic Sprague–Dawley (SD) rats weighing approximately 200 g were provided by the Animal Center of Southwest Medical University, Luzhou, China. Fifty rats were used to establish the MI models by ligation of the left anterior descending coronary artery; four rats died during the operation, and seven rats died after removal from the ventilator. The remaining 39 MI rats were randomly assigned to the MI, low-EMPA, and high-EMPA groups. Ten rats were assigned to the Sham group. All the rats were housed in an experimental animal house at the Heart Research Institute of Southwest Medical University. The feeding room was kept quiet, maintained at approximately 25 °C with 40–50% humidity, and a 12-h day and night cycle. Feed and water intake of the rats were not restricted, and the padding was changed regularly. All animal procedures conformed to the Guide for the Care and Use of Laboratory Animals published by the US National Institute of Health (8th edition, 2011) and were approved by the Institutional Animal Care and Treatment Committee of Southwest Medical University, China.
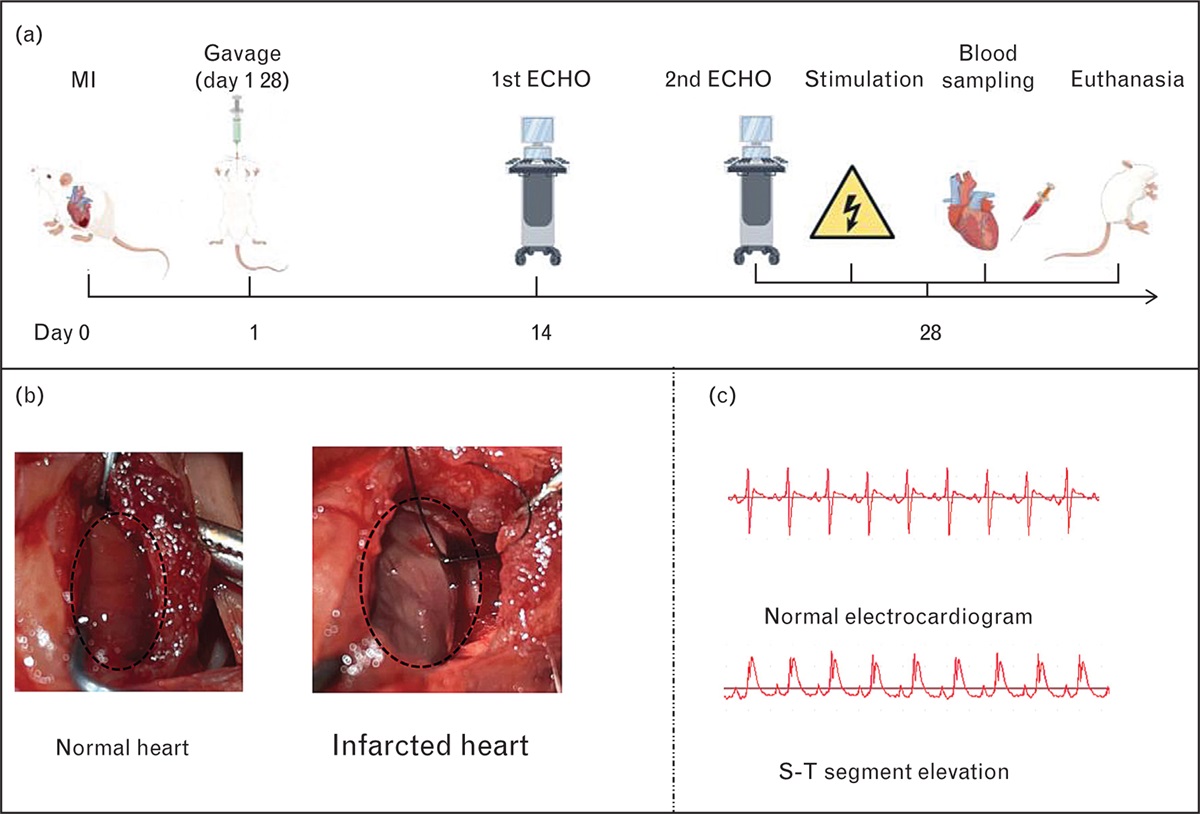
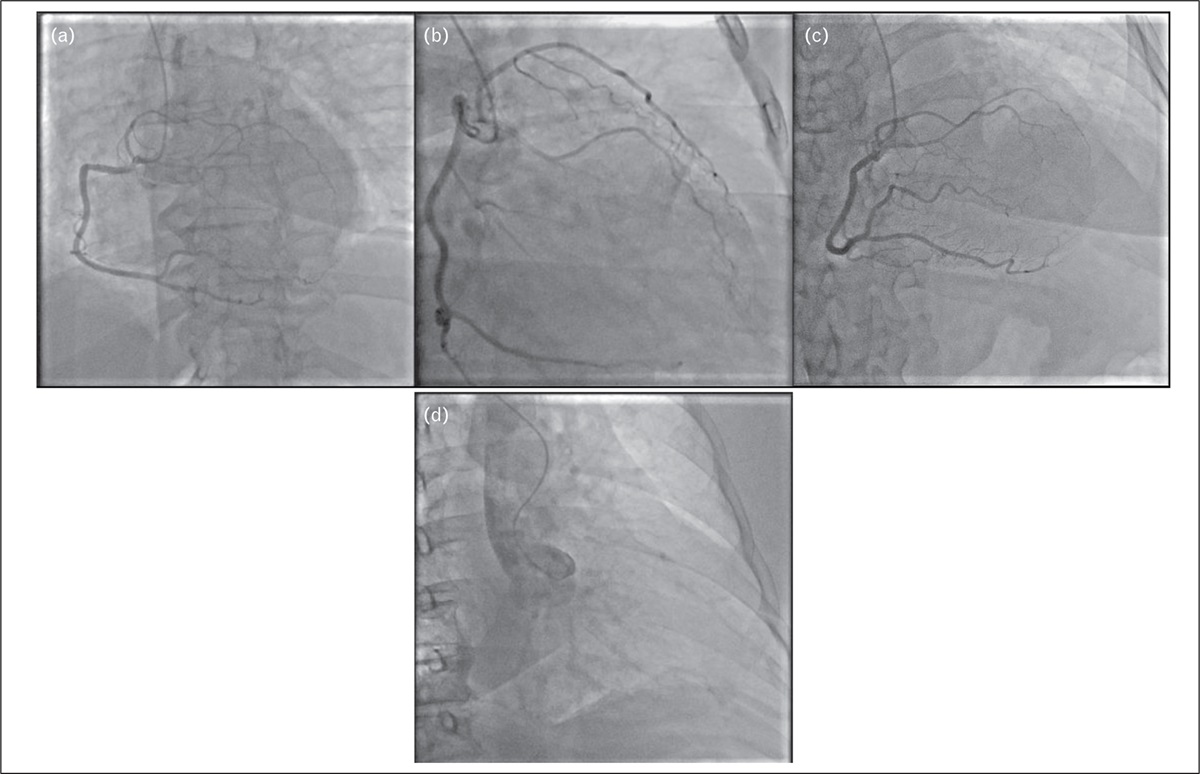
Animal treatmentAfter feed-only fasting for 12 h, the rats were anesthetized with an intraperitoneal injection of sodium pentobarbital (50 mg/kg) and fixed on the operating table for skin preparation and disinfection. Endotracheal intubation was performed from the oral cavity, and a ventilator was connected for mechanical ventilation (tidal volume 0.8 ml, respiratory rate, 80 beats/min; respiratory time ratio, 5 : 4). Electrocardiographic electrodes were inserted under the skin of the rat limbs, and the electrocardiogram was recorded using standard leads I, II, and a ventricular fibrillation. A longitudinal skin incision was made on the left thorax. The muscle was bluntly separated layer-by-layer and a thoracotomy was performed in the fourth intercostal space, after which the pericardium was separated, and the heart was exposed. The ligation point was 2 mm below the intersection of the pulmonary conus and the left atrial appendage, and ligation was performed with a 6-0 suture. A change in myocardial color from red to white (Fig. 1b) or S-T segment elevation was a sign of successful modeling (Fig. 1c). Rats in the Sham group underwent thoracotomy without ligation, and the chest was closed layer-by-layer.
 Fig. 1:
Fig. 1: Signs of successful modeling. (a) Experimental flow chart. (b) The myocardial color changed from red to white. (c) S-T segment was elevated.
The rats were administered a gavage on the day after the model was established. The rats in the low-EMPA group were intragastrically administered EMPA (10 mg/kg/day; Jardiance, Boehringer Ingelheim International GmbH, Germany), whereas those in the high-EMPA were intragastrically administered EMPA (30 mg/kg/day). Rats in the Sham and MI groups were intragastrically administered 3 ml of water. The drug was administered for 28 days.
EchocardiographyIn the second and fourth weeks after skin preparation, left ventricular posterior wall thickness (LVPWT), left ventricular anterior wall thickness (LVAWT), interventricular septum thickness (IVST), left ventricular end-diastolic diameter (LVEDD), left ventricular end-systolic diameter (LVESD), and left ventricular ejection fraction (LVEF) were measured using small animal echocardiography (Vevo2100 Small animal echocardiography, FUJIFILM, Japan) under gaseous anesthesia with isoflurane (anesthesia maintenance concentration 1.5%; Fig. 2a).
 Fig. 2:
Fig. 2: Structural changes in the heart measured by using M-mode echocardiography. EMPA treatment ameliorated structural changes in the hearts of MI rats, especially the low-dose EMPA. (a) Images of the ultrasonic cardiogram. (b) LVAW. (c) LVEDD. (d) LVPW. (e) LVEDS. (f) IVS. (g) EF. (h) Masson's staining of myocardial fibrosis. The data are presented as the mean ± SD. n1 (Sham group) = 10; n2 (MI group) = 10; n3 (low-EMPA group) = 11; n4 (high-EMPA group) = 12. Two-way repeated measure ANOVA was performed. ∗Means P < 0.05. ANOVA, analysis of variance; EF, ejection fraction; EMPA, empagliflozin; IVS, interventricular septum; LVAW, left ventricular anterior wall; LVEDD, left ventricular end-diastolic diameter; LVPW, left ventricular posterior wall; MI, myocardial infarction.
Electrical stimulationAfter anesthesia, skin preparation, mechanical ventilation, and thoracotomy as previously described, a bipolar pacemaker electrode was inserted into the peripheral area of the MI in rats at a depth of 1 mm, with a 2-mm interval between the two electrodes, and the electrodes were within 3 mm of the edge of the infarction. Burst stimulation was applied using a multiguide electrocardiograph recording stimulation system (60 ms in circumference, 10 ms in pulse width, 30 s in duration; NIHON KOHDEN), followed by stimulation for 1 min. The pacing voltage was started at 4 V and was increased by 1 V each time, with the threshold of ventricular fibrillation (Fig. 3b) being the lowest intensity that caused ventricular fibrillation.
 Fig. 3:
Fig. 3: Electrical stimulation. (a) High-dose EMPA significantly increased the ventricular fibrillation threshold of MI rats. The data are presented as the mean ± SD. n1 (Sham group) = 10; n2 (MI group) = 10; n3 (low-EMPA group) = 11; n4 (high-EMPA group) = 12. Two-way repeated measures ANOVA was performed. ∗Means P < 0.05. (b) Electrocardiogram of ventricular fibrillation after electrical stimulation. ANOVA, analysis of variance; EMPA, empagliflozin; MI, myocardial infarction.
ELISABlood samples were collected from the apex cordis after electrical stimulation, allowed to coagulate naturally at room temperature for 15 min, and centrifuged at 3000 rpm for 20 min. Rats were euthanized by exsanguination via transcardial perfusion with 50 ml of PBS, followed by heart excision. The blood noradrenaline levels were measured using ELISA (Rat, no.JM-01962R1-96T, Jiangsu Jingmei Biotechnology Co., LTD, Jiangsu, China) according to the manufacturer's instructions. Blood NE levels are expressed as ng/ml. All the experiments were performed four times.
Histological studies Hematoxylin–eosin and Masson's stainingLeft ventricular (LV) tissues were fixed with 4% tissue fixation solution for 24 h, dehydrated, embedded, and sectored (5-μm thickness), and then stained with HE/Masson's stain according to the standard protocols. The images were captured using a digital imaging system. The results of Masson's staining were analyzed using ImageJ software at 20× magnification.
ImmunohistochemistryAfter deparaffinization, rehydration, and permeabilization, the LV sections were immersed in 3% H2O2 for 10 min to inactivate endogenous peroxidase activity, and then rinsed with PBS three times for 5 min each. The sections were blocked with the 10% goat serum for 10 min at room temperature and then incubated with the anti-growth-associated protein 43 (GAP43) antibody (1 : 1000, ab75810, Abcam, Cambridge, UK) or the anti-tyrosine hydroxylase antibody (1 : 1000, ab112, Abcam) in 3% goat serum/1% BSA at 4 °C overnight. After rinsing with PBS three times, for 5 min each, the sections were incubated with the biotin-labeled goat antirabbit secondary antibody (1 : 1000, 7074P2, Cell Signaling Technology, Boston, USA) in 3% goat serum/1% BSA for 45 min at 37 °C, and then rinsed with PBS three times, 5 min each. DAB was used for color display and the sections were rinsed with tap water, re-stained with hematoxylin, dehydrated with gradient alcohol, permeabilized with xylene, and sealed with gum. Neural density was analyzed and measured using ImageJ software at 40× magnification.
Western blottingProteins were extracted from the margin of the LV infarction, and the protein concentration of the samples was measured using a BCA kit (P0010, Beyotime, Shanghai, China). The proteins in the samples were diluted to 5 mg/ml using RIPA lysis buffer (P0013B, Beyotime) and 6× SDS-PAGE protein loading buffer (P0015F, Beyotime). The samples were boiled for 10 min at 100 °C. Thereafter, 10% gels (PG112, EpiZyme, USA) were prepared, and 10 μl of the sample was added to each sample well. Electrophoresis (Bio-rad, California, USA) was performed at 80 V. After the proteins entered the lower layer, electrophoresis was performed at 150 V for 40 min. The PVDF membrane was activated by methanol, and a sandwich structure was created according to the direction of the positive and negative poles. Proteins were transferred onto the PVDF membrane for 90 min at 250 mA in transfer buffer. After sealing with protein-free rapid blocker for 15 min, the PVDF membrane was incubated with the primary antibodies, anti-NGF antibody (1 : 1000, ab52918, Abcam), anti-TrkA antibody (1 : 500, abs148274, Absin, Shanghai, China) anti-GAP43 antibody (1 : 1000, ab75810, Abcam), or anti-TH antibody (1 : 1000, ab112, Abcam), at 4 °C overnight. After rinsing with TBST three times for 10 min each, the PVDF membrane was incubated with goat antirabbit secondary antibody (1 : 1000, 7074P2, Cell Signaling Technology) for 90 min at room temperature. After rinsing with TBST three times for 10 min each, immunoreactive bands were detected using a chemiluminescent reagent (P0018AS, Beyotime). The procedures for measuring GAPDH (1 : 2000, ab181602, Abcam) were the same as in previous procedures, and the protein bands were scanned and quantified using ImageJ software.
Statistical analysisSPSS 17.0 statistical software was used for data processing, and the measurement data were expressed in the form of X ± SD. Two-way repeated measures ANOVA was used for comparison between groups, and P less than 0.05 was considered statistically significant.
Results Survival conditionDuring the gavage period, all rats in the Sham group survived. Three rats in the MI group, two in the low-EMPA group, and one in the high-EMPA group died.
EchocardiographyStructural changes in the rat hearts were measured using M-mode echocardiography during the second and fourth weeks. The key parameters measured are shown in Fig. 2. In general, in addition to LVPW, EMPA treatment significantly ameliorated the structural changes in LV in rats, and interestingly, the effect of low-dose EMPA was more significant. LVAW was ameliorated in both the low-EMPA and high-EMPA groups (Fig. 2b) compared with the MI group (P< 0.05), and the difference between the low-EMPA and the high-EMPA groups was not statistically significant (P> 0.05). The LVPW in all groups showed no significant differences (P < 0.05) (Fig. 2c). Compared with the MI group, low-dose EMPA significantly ameliorated LVEDS, LVEDD, and IVS (Fig. 2d–f) at both the second and fourth weeks (P< 0.05). High EMPA also significantly ameliorated the three parameters at the fourth week (P< 0.05); however, the effect of high-dose EMPA was not significant in the second week (P> 0.05). Compared with the MI group, both the high-EMPA and low-EMPA groups showed a significant improvement in ejection fraction (Fig. 2g; P< 0.05), and there was no difference between the effect of high-EMPA and low-dose EMPA (P< 0.05). Masson's staining showed that the overall LV fibrosis area in MI rats was significantly increased (P< 0.05; Fig. 2h). EMPA treatment decreased myocardial fibrosis in MI rats (P< 0.05) and high-dose EMPA treatment decreased the myocardial fibrosis area more significantly, but the antifibrosis effect in the low-EMPA and high-EMPA groups was not statistically significant (P> 0.05).
Ventricular fibrillation thresholdCompared with the MI group, the ventricular fibrillation threshold in the high-EMPA group was significantly increased (P < 0.05). Low-dose EMPA slightly improved the ventricular fibrillation threshold, but this was not statistically different from that observed in the MI group (P> 0.05; Fig. 3a).
Sympathetic activitySympathetic activity and NE levels in the blood were measured by ELISA, and the results are shown in Fig. 4. Compared with the MI group, high-dose EMPA significantly decreased the level of NE in the blood of MI rats (P < 0.05). Low-dose EMPA slightly decreased sympathetic activity, but the decrease was not statistically different compared with the MI group (P > 0.05).
 Fig. 4:
Fig. 4: Sympathetic activity and the levels of NE in the blood. EMPA treatment inhibited sympathetic activity. The data are presented as the mean ± SD. n1 (Sham group) = 10; n2 (MI group) = 10; n3 (low-EMPA group) = 11; n4 (high-EMPA group) = 12. Two-way repeated measures ANOVA was performed. ∗Means P less than 0.05. ANOVA, analysis of variance; EMPA, empagliflozin; MI, myocardial infarction.
HistomorphologyAs shown in Fig. 5, HE staining showed that myocardial atrophy, karyopyknosis, diffuse vacuolation of subendocardial cardiomyocytes, and inflammatory cell infiltration were observed in MI rats compared with normal rats. Thus, EMPA can improve MI-related histomorphological changes.
 Fig. 5:
Fig. 5: Empagliflozin ameliorated myocardial atrophy, karyopyknosis, diffuse vacuolation of subendocardial cardiomyocytes, and inflammatory cells infiltration in MI rats. High-dose EMPA was more effective than low-dose EMPA. EMPA, empagliflozin; MI, myocardial infarction.
Levels of the neural remodeling indicators nerve growth factor, tyrosine kinase receptor A, growth-associated protein 43, and tyrosine hydroxylaseThe results for GAP43 and tyrosine hydroxylase are shown in Fig. 6. According to previous studies,17,18 the infarct area undergoes denervation, and the infarct margin area undergoes sympathetic remodeling after MI. Compared with the Sham group, the distribution of GAP43-positive and tyrosine hydroxylase-positive sympathetic fibers with coarse diameters was disordered, and fiber density was increased in the margin of the infarct area. As shown in Fig. 6a, EMPA treatment significantly attenuated sympathetic remodeling after MI; the density of GAP43-positive and tyrosine hydroxylase-positive sympathetic fibers was reduced significantly in the high-EMPA and low-EMPA groups (P < 0.05), and the effect of high-dose EMPA was more significant than that of the low-dose (P< 0.05). Results of Western blotting (Fig. 6b) showed that high-dose EMPA significantly decreased the expression of NGF, TrkA, GAP43, and tyrosine hydroxylase (P< 0.05). Low-dose EMPA significantly decreased NGF and TrkA expression (P< 0.05) and slightly decreased the expression of GAP43 and tyrosine hydroxylase, but the difference was not statistically significant between the MI and low-EMPA groups (P> 0.05). Compared with the low-EMPA group, the expression of these proteins was ‘numerically lower’ without a significant difference in the high-EMPA group (P> 0.05).
 Fig. 6:
Fig. 6: Empagliflozin treatment reduced sympathetic remodeling in myocardial infarction rats; the effect of the high-dose empagliflozin was more significant. (a) Presence of TH and GAP43 measured by IHC. (b) WB results of GAP43 and TH. The data are presented as the mean ± SD. n1 (Sham group) = 10; n2 (MI group) = 10; n3 (low-EMPA group) = 11; n4 (high-EMPA group) = 12. Two-way repeated measures ANOVA was performed. ∗Means P < 0.05. ANOVA, analysis of variance; EMPA, empagliflozin; IHC, immunohistochemistry; SD, standard deviation; TH, tyrosine hydroxylase; WB, Western blotting.
Discussion Empagliflozin ameliorated the occurrence of ventricular arrhythmias by attenuating sympathetic remodeling and sympathetic activity after myocardial infarctionOur data showed that EMPA increased the threshold of ventricular fibrillation in MI rats, and the effect of high-dose EMPA was significant, while that of low-dose EMPA was minimal. Thus, a high dose of EMPA could significantly reduce the incidence of ventricular arrhythmias after MI. This is consistent with the conclusions of previous reports. Azam et al.16 found that, compared with the Langendorff perfusion with physiological saline, the Langendorff perfusion with EMPA (1 μl) could significantly reduce the induction rate of ventricular fibrillation greater than 10 s in ischemic isolated rabbit hearts (16.7 ± 3.3 vs. 60 ± 8.7% in control hearts, P= 0.003). Wang et al.19 found that DAPA significantly reduced the induction rate of ventricular arrhythmias in rats with isoproterenol-induced cardiomyopathy. However, Fernandes et al. conducted a meta-analysis of 14 clinical trials involving 49 963 patients with type 2 diabetes and/or heart failure and found that the incidence of ventricular arrhythmias did not decrease significantly compared with the control group [odds ratio (OR) 0.85; 95% confidence interval (CI), 0.66–1.11; P= 5.23], but the incidence of sudden cardiac death decreased by 28%.20 Our data also showed that EMPA significantly reduced the expression of NGF and TrkA, the density of tyrosine hydroxylase-positive and GAP43-positive fibers at the margin of infarction, and the blood concentration of NE. The effect of high-dose EMPA was more significant; thus, EMPA dose-dependently reduced sympathetic remodeling and sympathetic activity after MI. Wan et al.21 claimed that SGLT2i could significantly ameliorate blood pressure but had no effect on heart rate, which may be achieved through its effect on sympathetic nerves. A previous report also confirmed that SGLT2i can reduce sympathetic activity in a normoglycemic mouse model.22 Zhang et al.23 also found that DAPA could significantly ameliorate the concentration of NE in the blood of HFpEF pig models. However, there are few reports on whether SGLT2i can regulate sympathetic remodeling. Current clinical trials have found no correlation between SGLT2i and ventricular arrhythmia occurrence. Detailed research is required to investigate whether SGLT2i can be used to reduce sympathetic remodeling after MI, and thus ameliorate the occurrence of ventricular arrhythmias.
Empagliflozin ameliorated the occurrence of ventricular arrhythmias by improving cardiac function and cardiac structural remodeling after myocardial infarctionMany studies have confirmed that SGLT2i significantly improves cardiac function in patients with heart failure.8–10 Yu et al.24 reported that SGLT2is improved left atrial adverse remodeling and reduced patient mortality in patients with type 2 diabetes and HFrEF. Zhang et al.25 found after a meta-analysis of 13 randomized controlled trials involving 1251 patients with T2DM and/or heart failure that SGLT2is significantly reversed cardiac remodeling, improving LV systolic and diastolic function, LV mass and volume, especially in patients with HFrEF and among those taking empagliflozin compared with other SGLT2i. Our study confirmed that EMPA significantly improved the cardiac function in MI rats. The results of the ultrasonic cardiogram showed that, compared with the Sham group, the cardiac function of MI rats was worse, including decreased LVEF, LVAW, and IVS, and increased LVEDS and LVEDD. EMPA treatment significantly improved the cardiac function in MI rats, particularly in low-EMPA rats. HE staining showed that EMPA reduced the infarct size in the ischemic area of MI rats. To further explore the reasons for the above effect, we performed Masson's staining of the myocardium, and the results showed that EMPA significantly decreased myocardial fibrosis; however, the results of the echocardiography showed that low-dose EMPA had a better effect. Myocardial fibrosis is a sign of cardiac structural remodeling and is the basis for the occurrence and persistence of arrhythmias.26,27 The results of Masson's staining were consistent with previous results; EMPA affects fibrosis by inhibiting the TGF-β/Smad-signaling pathway in nondiabetic rats after MI.28 DAPA has also been shown to reduce myocardial fibroblast infiltration and fibrosis after MI in mice.29 The antifibrosis effect of SGLT2i has also been observed in other animal models of heart failure and type 2 diabetes.30,31 And Li et al.32 found that SGLT2i alleviated the epicardial adipose tissue inflammation and atrial fibrosis in atrial fibrillation rats. SGLT2i can significantly ameliorate cardiac structural remodeling in cardiac diseases such as MI and heart failure. However, whether SGLT2i, such as ACEI/ARB, can be routinely used to improve cardiac structural remodeling in the MI setting still needs to be confirmed in a large number of trials.
Study limitationsEchocardiography results showed that the low-dose group had more significant effects on cardiac structural changes and function in MI rats than the high-dose group, although some indicators were not statistically significant between the two groups. This article does not continue to deeply study its mechanism, which is the limitation of this article.
ConclusionEMPA alleviated the occurrence of ventricular arrhythmias after MI by improving cardiac function and cardiac structural remodeling. This improvement may be related to a reduction in sympathetic activity and inhibition of the NGF/TrkA pathway, thereby inhibiting sympathetic remodeling. This study provides an animal experimental basis for clinical treatment of ventricular arrhythmias after MI.
AcknowledgementsThe authors thank Dr Xiaoqiu Tan (Key Laboratory of Medical Electrophysiology of Ministry of Education and Medical Electrophysiological Key Laboratory of Sichuan Province, Collaborative Innovation Center for Prevention and Treatment of Cardiovascular Disease, Institute of Cardiovascular Research, Southwest Medical University) for providing the experimental platform.
Ethics approval and consent to participate: All animal procedures conformed to Guide for Care and Use of Laboratory Animals published by US National Institute of Health (8th edition, 2011) and were approved by the Institutional Animal Care and Treatment Committee of Southwest Medical University, China.
Consent for publication: Not applicable.
Availability of data and materials: The data used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Funding: This research was funded by the fund of Medical Research project of Sichuan Province (S21111).
Authors’ contributions: Y.J. is responsible for designing experiments, doing experiments and writing article. Y.D. and H.F. are responsible for doing experiments. Ta.L. is responsible for guiding the experiment. Ti.L. is responsible for reviewing the article. Q.Y. is responsible for designing experiments, guiding the experiment, and reviewing the article.
Conflicts of interestThere are no conflicts of interest.
References 1. Cao JM, Chen LS, KenKnight BH, et al. Nerve sprouting and sudden cardiac death. Circ Res 2000; 86:816–821. 2. Chen PS, Chen LS, Cao JM, Sharifi B, Karagueuzian HS, Fishbein MC. Sympathetic nerve sprouting, electrical remodeling and the mechanisms of sudden cardiac death. Cardiovasc Res 2001; 50:409–416. 3. Zhou Z, Liu C, Xu S, et al. Metabolism regulator adiponectin prevents cardiac remodeling and ventricular arrhythmias via sympathetic modulation in a myocardial infarction model. Basic Res Cardiol 2022; 117:34. 4. Enomoto M, Mantyh PW, Murrell J, Innes JF, Lascelles BDX. Antinerve growth factor monoclonal antibodies for the control of pain in dogs and cats. Vet Rec 2019; 184:23. 5. Marlin MC, Li G. Biogenesis and function of the NGF/TrkA signaling endosome. Int Rev Cell Mol Biol 2015; 314:239–257. 6. Kohn J, Aloyz RS, Toma JG, et al. Functionally antagonistic interactions between the TrkA and p75 neurotrophin receptors regulate sympathetic neuron growth and target innervation. J Neurosci 1999; 19:5393–5408. 7. Zelniker TA, Braunwald E. Mechanisms of cardiorenal effects of sodium-glucose cotransporter 2 inhibitors: JACC state-of-the-art review. J Am Coll Cardiol 2020; 75:422–434. 8. Zelniker TA, Wiviott SD, Raz I, et al. SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet 2019; 393:31–39. 9. Zannad F, Ferreira JP, Pocock SJ, et al. SGLT2 inhibitors in patients with heart failure with reduced ejection fraction: a meta-analysis of the EMPEROR-Reduced and DAPA-HF trials. Lancet 2020; 396:819–829. 10. McMurray JJV, Solomon SD, Inzucchi SE, et al. DAPA-HF Trial Committees and Investigators. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med 2019; 381:1995–2008. 11. Mosenzon O, Wiviott SD, Cahn A, et al. Effects of dapagliflozin on development and progression of kidney disease in patients with type 2 diabetes: an analysis from the DECLARE-TIMI 58 randomised trial. Lancet Diabetes Endocrinol 2019; 7:606–617. 12. De Marzo V, Savarese G, Porto I, Metra M, Ameri P. Efficacy of SGLT2-inhibitors across different definitions of heart failure with preserved ejection fraction. J Cardiovasc Med (Hagerstown) 2023; 24:537–543. 13. Huang Y, Fang C, Zhang Y, Ma L, Zhou H, Ye H. Effectiveness and safety of angiotensin receptor-neprilysin inhibitor and sodium-glucose cotransporter-2 inhibitors for patients with heart failure with reduced ejection fraction: a meta-analysis. J Cardiovasc Med (Hagerstown) 2023; 24:123–131. 14. Pagnesi M, Baldetti L, Aimo A, et al. Prognostic benefit of new drugs for HFrEF: a systematic review and network meta-analysis. J Clin Med 2022; 11:348. 15. Zelniker TA, Bonaca MP, Furtado RHM, et al. Effect of dapagliflozin on atrial fibrillation in patients with type 2 diabetes mellitus: insights from the DECLARE-TIMI 58 Trial. Circulation 2020; 141:1227–1234. 16. Azam MA, Chakraborty P, Si D, et al. Antiarrhythmic and inotropic effects of empagliflozin following myocardial ischemia. Life Sci 2021; 276:119440. 17. Cao JM, Fishbein MC, Han JB, et al. Relationship between regional cardiac hyperinnervation and ventricular arrhythmia. Circulation 2000; 101:1960–1969. 18. Zhou S, Chen LS, Miyauchi Y, et al. Mechanisms of cardiac nerve sprouting after myocardial infarction in dogs. Circ Res 2004; 95:76–83. 19. Wang FZ, Wei WB, Li X, et al. The cardioprotective effect of the sodium-glucose cotransporter 2 inhibitor dapagliflozin in rats with isoproterenol-induced cardiomyopathy. Am J Transl Res 2021; 13:10950–10961. 20. Fernandes GC, Fernandes A, Cardoso R, et al. Association of SGLT2 inhibitors with arrhythmias and sudden cardiac death in patients with type 2 diabetes or heart failure: a meta-analysis of 34 randomized controlled trials. Heart Rhythm 2021; 18:1098–1105. 21. Wan N, Rahman A, Hitomi H, Nishiyama A. The effects of sodium-glucose cotransporter 2 inhibitors on sympathetic nervous activity. Front Endocrinol (Lausanne) 2018; 9:421. 22. Liu Y, Wu M, Xu B, Kang L. Empagliflozin alleviates atherosclerosis progression by inhibiting inflammation and sympathetic activity in a normoglycemic mouse model. J Inflamm Res 2021; 14:2277–2287. 23. Zhang N, Feng B, Ma X, Sun K, Xu G, Zhou Y. Dapagliflozin improves left ventricular remodeling and aorta sympathetic tone in a pig model of heart failure with preserved ejection fraction. Cardiovasc Diabetol 2019; 18:107. 24. Yu S, Sun Y, Wang N, et al. Effect of sodium-glucose cotransporter 2 inhibitors on left atrial remodeling and prognosis in patients with type 2 diabetes and heart failure with reduced ejection fraction. J Cardiovasc Med (Hagerstown) 2023; 24:829–837. 25. Zhang N, Wang Y, Tse G, et al. Effect of sodium-glucose cotransporter-2 inhibitors on cardiac remodelling: a systematic review and meta-analysis. Eur J Prev Cardiol 2022; 28:1961–1973. 26. Moreira LM, Takawale A, Hulsurkar M, et al. Paracrine signalling by cardiac calcitonin controls atrial fibrogenesis and arrhythmia. Nature 2020; 587:460–465. 27. Dzeshka MS, Lip GY, Snezhitskiy V, Shantsila E. Cardiac fibrosis in patients with atrial fibrillation: mechanisms and clinical implications. J Am Coll Cardiol 2015; 66:943–959. 28. Daud E, Ertracht O, Bandel N, et al. The impact of empagliflozin on cardiac physiology and fibrosis early after myocardial infarction in nondiabetic rats. Cardiovasc Diabetol 2021; 20:132. 29. Lee TM, Chang NC, Lin SZ. Dapagliflozin, a selective SGLT2 Inhibitor, attenuated cardiac fibrosis by regulating the macrophage polarization via STAT3 signaling in infarcted rat hearts. Free Radic Biol Med 2017; 104:298–310. 30. Santos-Gallego CG, Requena-Ibanez JA, San Antonio R, et al. Empagliflozin ameliorates diastolic dysfunction and left ventricular fibrosis/stiffness in nondiabetic heart failure: a multimodality study. JACC Cardiovasc Imaging 2021; 14:393–407. 31. Tian J, Zhang M, Suo M, et al. Dapagliflozin alleviates cardiac fibrosis through suppressing EndMT and fibroblast activation via AMPKα/TGF-β/Smad signalling in type 2 diabetic rats. J Cell Mol Med 2021; 25:7642–7659. 32. Li L, Hua C, Liu X, et al. SGLT2i alleviates epicardial adipose tissue inflammation by modulating ketone body-glyceraldehyde-3-phosphate dehydrogenase malonylation pathway. J Cardiovasc Med (Hagerstown) 2023; 24:232–243.
Comments (0)