
Remember me






We enrolled 302 patients diagnosed over a period of 23 years, 58.6% of whom were female. The JIA categories included 27.4% (83) oligoarthritis (OligoJIA), 17.9% (54) RF-polyarticular JIA (RF-pJIA), 5% (15) RF + polyarticular JIA (RF + pJIA), 7% (16) PsJIA, 18.2% (55) ERA, 18.9% (57) systemic JIA (SJIA), and 5.6% (17) undifferentiated arthritis. Our results are similar to the findings by Al Mayouf and colleagues in their study that found oligoarticular JIA to be the most predominant form of JIA in Africa and Middle East [13]. However, in our study, the countries in sub-sahara Africa had a higher proportion of systemic JIA and polyarticular JIA. This implies that there may be regional differences or the children with the more aggressive forms of the disease are the ones who seek care at these facilities. More data will be required to ascertain if these differences are significant. Due to under-representation of certain regions in Africa, a critical first step would be empowering the workforce in these regions to identify and manage JIA patients. This would help in generating data to inform practice. To substantiate the existence of a genuinely distinct subtype profile among African countries, further comprehensive epidemiologic data is imperative, given the current dearth of data in our continent.
The epidemiological data of enrolled patients in the registry is similar to various other research articles on JIA patients, particularly in terms of gender distribution and category prevalence [13,14,15]. However, our findings reveal a notable disparity among African countries concerning the age at inclusion and diagnosis delay. Despite Oligo-articular JIA being the most predominant category, the median age at diagnosis was 7 years yet the peak age for this category is 2–4 years [21]. In Kenya and Nigeria where polyarticular JIA was among the predominant categories, the median age was 9 and 12 years respectively yet biphasic peaks are reported globally of 1–4 years and 6–12 years [21]. Egypt exhibits a lower diagnosis delay compared to other countries. This observed distinction correlates with the high number of the rheumatology workforce in Egypt compared to other countries in Africa. This trend is similar to other studies across the globe [10,11,12, 17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38].
Figure 2 illustrates the African member state countries that are members of the PAFLAR research working group and those that participated in our PAFLAR registry. This mirrors the countries with paediatric rheumatology centres as highlighted in one of our previous publications [8].
Fig. 2
PAFLAR’s JIA registry activity in Africa. Red - Countries with PAFLAR research members contributing to the JIA Registry through subcommittees: Scientific, Ethics, Investigation Coordination, and Data Management & Manuscripts. Green - These African countries are either undergoing or have completed induction to become co-investigators in the registry. Those that have completed induction are awaiting ethical approvals before adding data. Blue - These five countries have obtained ethical approvals and have begun inputting data into the registry
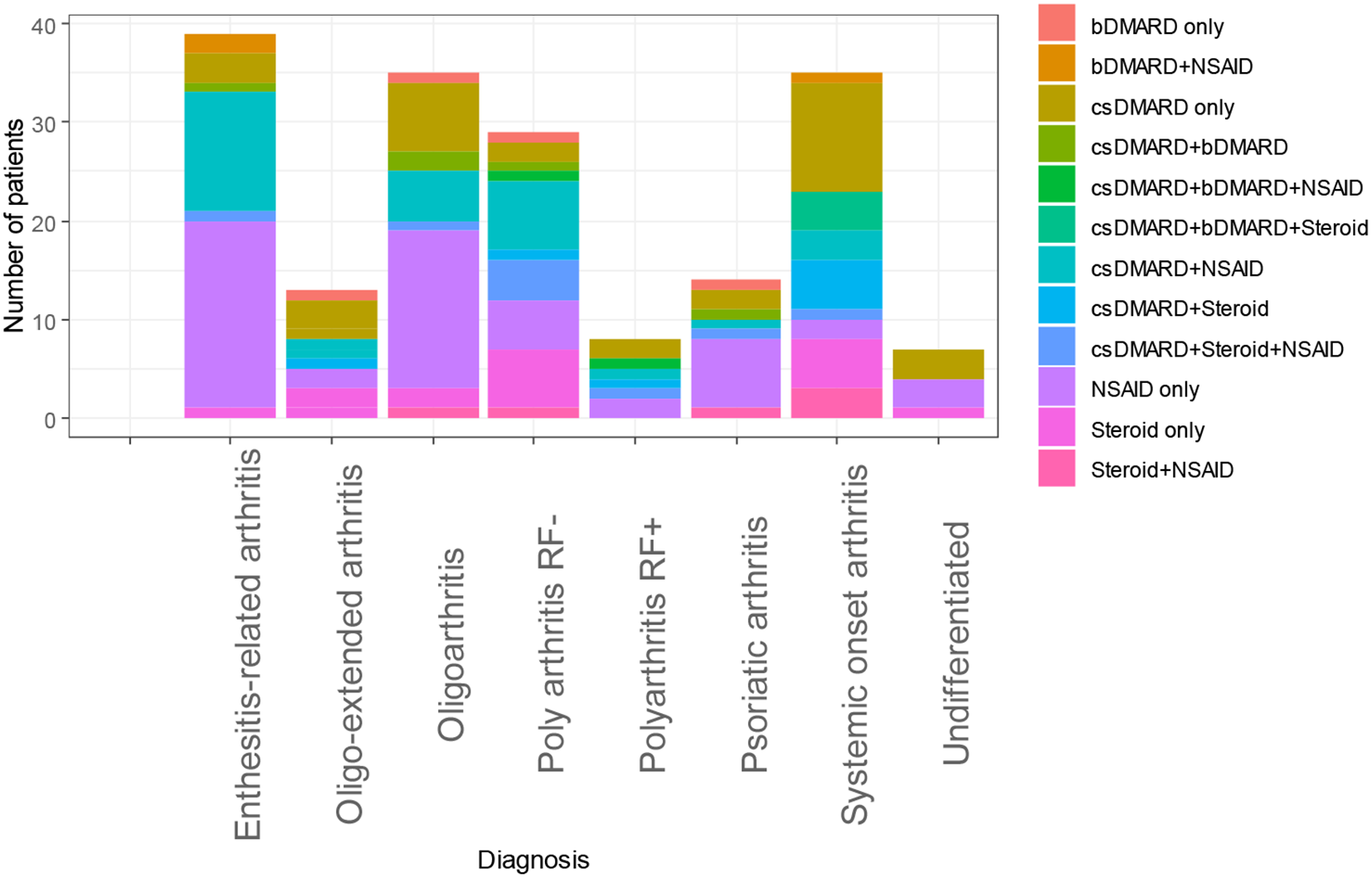
As regards treatment, the commonest therapies were NSAID therapy at 31.1%, synthetic DMARDs at 18.1%, synthetic DMARDs combined with NSAIDs at 17.5% and steroid therapy at 9.6%. Biological DMARDs accounted for 2.3% of therapies offered to our patients. The average JADAS score was 10.3 (range 3.8–17) and the average CHAQ score was 1.3 (range 0.65–1.95). Treatment options are influenced by the disease category and the medications available among other factors [39]. The predominant JIA category in our cohort was Oligoarticular JIA which might explain the predominantly high proportion of NSAID use. Nonetheless, the use of current synthetic and biological disease modifying antirheumatic drugs (DMARDs) requires more research on the optimal timing and duration applicable within our context [39]. Our findings reveal a limited overall utilization of biologics, accompanied by a considerable disparity in the usage patterns of steroids, NSAIDs, and csDMARDs within the studied cohort. This was highlighted in one of our previous publications that reveals the variation in availability of DMARD therapy and biological therapies [8]. This observed variation may be attributed to the economic conditions prevalent in African countries, further compounded by disparities in the distribution of categories within this demographic group. The discerned heterogeneity in medication utilization underscores the multifaceted nature of therapeutic decision-making processes within the context of the economic landscape and the diverse spectrum of JIA categories prevalent in this population.
In our cohort, we noted the lower frequency of uveitis compared to other international cohorts or registries. This was reiterated by Al Mayouf and co-authors who reported the incidence of uveitis and anti-nuclear antibody (ANA) positivity to be lower as compared to the incidence from other regions globally [13]. Addressing this disparity requires concerted efforts to implement routine screening for uveitis and enhance accessibility to ophthalmology care throughout our continent.
The absence of data pertaining to disease activity and functionality scores (CHAQ and JADAS) in certain countries is notable, as routine evaluation of these scores is not uniformly conducted across all centers. This emphasizes the imperative need for the implementation of strategic initiatives aimed at enhancing the capacity of healthcare professionals specializing in pediatric rheumatology throughout our continent to regularly assess and document the quality of life among JIA patients [40, 41]. The prospective segment of the PAFLAR registry, incorporating prospective follow-up data, is anticipated to address and rectify this existing gap.
As of the date of data extraction, the PAFLAR JIA registry had successfully enrolled 302 patients from eight centers across five African countries. However, this falls below our initial set target of enrolling all countries with paediatric rheumatology centres. We estimate we have 25 paediatric rheumatologists across Africa with Ethiopia being the most recent country to have its first paediatric rheumatologist. One of the challenges faced was the protracted and different requirements to obtain local ethical approval among various African member states. In addition, financial constraints made it difficult to compensate members for their time to input data hence we relied on their goodwill and willingness to support our registry. Some countries had strict data sharing laws which we postulate might have discouraged some members from enrolling patients into our registry. Another limitation we faced was that data collection was fragmented and partial hence limiting the epidemiological value of the study. Hence, among our 11 African member states only 5 participated in our PAFLAR JIA Registry. We hope to overcome some of these challenges by lobbying for more resources to support ethical approval applications and compensate members for their time and efforts in participation in our registry. We hope publication of this manuscript can help motivate other African member states to appreciate the importance of collective efforts in generating data and motivate them to participate in similar future initiatives. Nonetheless, our study provides insight on the profound heterogeneity of access to primary care and treatments in different countries across Africa.
We shall endeavor to continue with our social media and awareness campaign among our members to highlight the benefits of collaborative efforts and importance of participation in the PAFLAR JIA Registry. In view of this, we plan to administer a feedback survey amongst our research working group members to identify potential barriers affecting both patient and investigator recruitment. Our goal is to thoroughly understand these challenges and devise effective solutions to enhance enrollment in the PAFLAR JIA registry.
In order to overcome challenges in obtaining ethical approval, our ethics subcommittee actively engages with potential investigators, offering guidance and support to streamline the approval process with their respective local ethical committees. The aim is to navigate and address any variations or hurdles in ethical approval across different regions.
Recognizing the power of social media, we launched a dedicated campaign to raise awareness and attract potential participants. This initiative aims to tap into online platforms to disseminate information about the registry, creating a broader reach and engagement within the community.
Thus, to optimize recruitment we endeavour to implement a holistic approach combining multiple recruitment strategies and channels, tailoring communication with the native language of the target audience, being active (mobilize teams), reactive (provide prompt technical support), and proactive (share regular updates and reminders) [42]. Increasing awareness within the community about the existence of the registry and its potential outcomes could assist us in addressing these challenges [42].
Comments (0)