Study Design
This was a multicenter retrospective observational cohort study analyzing data from two comprehensive stroke centers (Neurocenter, Klinikum Stuttgart, Stuttgart, Germany, and Department of Neurology, Inselspital, Bern University Hospital and University of Bern, Bern, Switzerland). This study was approved by the local institutional review boards (Ethics Commission of the State Medical Association of Baden-Württemberg [F-2012-077]; Kantonale Ethikkommission Bern [231/14]). Additional approval and patient consent was required for inclusion in the EVT registry (Stuttgart). The study was conducted in accordance with the Declaration of Helsinki. The Strengthening the Reporting of Observational Studies in Epidemiology guidelines were used to ensure appropriate reporting of the findings from this retrospective observational study [23].
Study Population
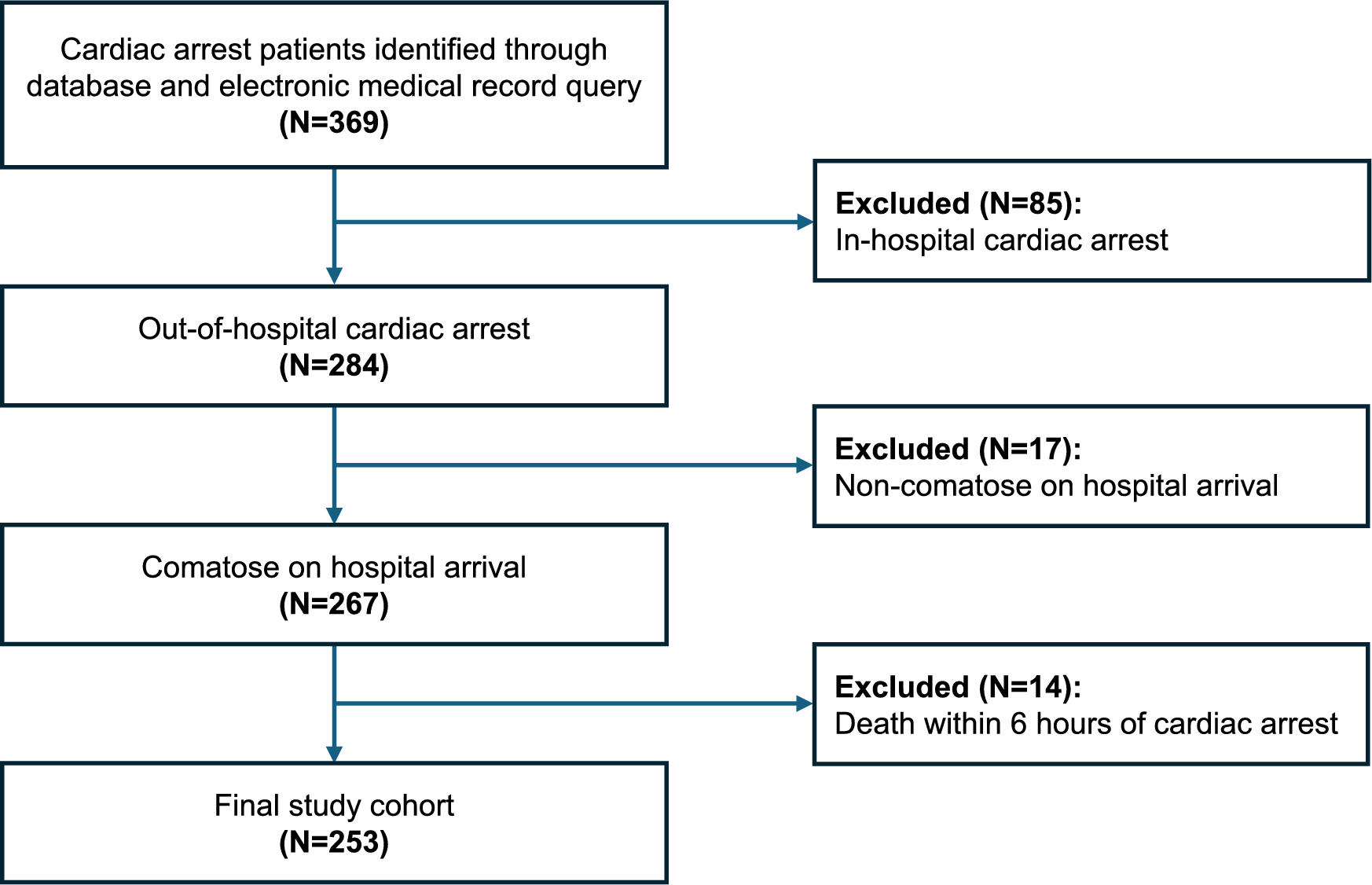
Consecutive patients diagnosed with CVST of any etiology, evaluated by digital subtraction angiography (DSA), and that required EVT treatment between January 2010 and December 2022 were identified retrospectively from an ongoing prospective single-center EVT registry (Stuttgart) and the national stroke registry (Swiss Stroke Registry, Bern). The Swiss Stroke Registry is an obligatory registry prospectively including all patients with stroke (ischemic stroke, ICH, and CVST). Within established neurovascular networks, patients could be diagnosed and treated at the respective stroke center, or they might have been transferred from surrounding hospitals for EVT or neurointensive care [24]. There were no standard operating procedures declaring EVT mandatory in certain predefined situations. Treatment decisions were made on a case-by-case basis by an interdisciplinary team (neurology, interventional neuroradiology, and neurosurgery). In general, EVT was considered in patients who presented with a suspected poor prognosis (coma with a Glasgow Coma Scale [GCS] score < 9, ICH, involvement of deep cerebral veins, large thrombus load, and/or rapid clinical deterioration before EVT despite adequate anticoagulation therapy) as a rescue strategy. The presence of these clinical factors alone did not facilitate the decision to perform early or late EVT. This decision was made by the treatment team (emergency department, stroke unit, neurointensive care, interventional neuroradiology, and neurosurgery), required an interdisciplinary consultation and was based on course of the disease (i.e., slow or rapid deterioration), additional imaging findings (e.g., brain edema, venous infarction), and capacities. Various endovascular strategies (e.g., aspiration or stent retriever thrombectomy, stent placement, percutaneous transluminal angioplasty, rheolytic thrombectomy, or thrombus fragmentation) were used based on the decision of the interventional neuroradiologist. Stent placement was considered an option in cases of repeated and/or complete reocclusion. Strategies could be adapted and combined during the course of the procedure. All patients with confirmed CVST were initially treated with continuous unfractionated heparin (bolus; anti-Xa-activity controlled [therapeutic range: 0.3–0.7 IU/ml]) followed by either unfractionated or low-molecular weight heparin (after EVT). In cases of stent placement, an additional dual platelet aggregation inhibition was installed (aspirin at 100 mg per day plus clopidogrel at 75 mg per day or ticagrelor at 90 mg twice daily). If the patient underwent EVT within the first 24 h of diagnosis, we considered this approach as first-line rescue treatment, given the limited time interval between the initiation of medical therapy and the procedure.
Patients were eligible for further analysis if the following criteria were met: (1) the patient was hospitalized with acute symptoms that could be directly attributed to CVST; (2) CVST was revealed by acute cerebral imaging (magnetic resonance imaging or computed tomography with contrast for those with contraindications); (3) documentation of a modified Rankin Scale (mRS) score at discharge and/or during follow-up 3 months after the index event. Because CVST predominantly affects younger patient populations, we did not apply a lower age limit. Exclusion criteria included (1) performance of a DSA study that did not lead to a subsequent EVT (e.g., chronic CVST or cerebral sinus stenosis without thrombosis); (2) incidental detection of a chronic CVST by DSA (which was performed due to other conditions such as arteriovenous malformations); and (3) lack of informed consent.
To evaluate the impact of time (i.e., the time elapsed between emergency consultation/hospitalization and the initiation of treatment), patients were subdivided into two groups: (1) patients who underwent treatment within 24 h (early EVT) and (2) patients who underwent treatment more than 24 h after hospitalization and diagnosis of CVST (late EVT). Because there were no data on the impact of earlier versus later EVT treatment in this patient population, we decided to use the assumed time to treatment initiation in the only published randomized controlled trial on EVT in CVST (Thrombolysis or Anticoagulation for Cerebral Venous Thrombosis [TO-ACT]) as a cutoff [16]. Given an interquartile range (IQR) for the time from diagnosis to randomization between 0 and 1 days (patients had to be randomized within 24 h after CVST diagnosis), and a median time from randomization to EVT of 4.5 h (278 [IQR 105–724] minutes) plus an unknown time from emergency consultation until final diagnosis, the assumed time to treatment initiation would be approximately 24 h.
Outcome parameters included functional independence (mRS score 0–2) at 90 days, mortality (mRS 6) at 3 months, in-hospital mortality, and functional independence (mRS score 0–2) at discharge.
Data Collection
Baseline characteristics (age, sex, medical history, symptom onset, physical examination, and mRS score) were extracted from the respective registries (PB and VH; both masked for the time elapsed between emergency consultation and EVT) and—if required—retrospectively completed according to emergency department admission notes, referral papers, and/or discharge letters. For the scope of this article, we distinguished between coma (GCS < 9) and somnolence/stupor (GCS 9–14). Imaging data were stored and analyzed in our picture archiving and communications system. We used the reports of the original read in order to describe imaging findings, such as ICH or subarachnoid hemorrhage (SAH), venous congestion, venous infarction, or thrombus load, as well as the number and location of the involved sinus(es). These findings were acquired retrospectively and verified in an additional read prior to this analysis (VH). Partial recanalization after EVT was defined as recanalization of one or more affected sinuses (but not all; residual thrombus material). In both centers, outcome data were recorded prospectively during scheduled follow-up consultations. A trained and specialized study nurse (trained in neuroradiology and neurology) collected the 3-month follow-up data on functional outcomes (mRS) and mortality via telephone calls (Stuttgart). Follow-up visits were scheduled 3 months after the index event in the outpatient department (Bern).
Statistical Analysis
Numerical baseline characteristics were described using the median (± IQR) or mean (± standard deviation [SD]). Frequencies were used to present categorical parameters. Group comparisons of categorical parameters were performed using the Fisher exact t-test or the χ2 test. The Kruskal–Wallis test or the Mann–Whitney U-test were applied as appropriate to evaluate numerical (outcome) parameters. The comparison of outcome variables was reported using odds ratios (ORs) and 95% confidence intervals (CIs) with adjustment in case of significant differences in baseline characteristics. A p value of < 0.05 was considered statistically significant. Statistical analyses were performed using STATA/IC 13.1 for Windows (StataCorp, College Station, TX).
Multivariate logistic regression was performed in order to determine factors associated with good functional outcome. Because of sample size restrictions, we could only include a small number of covariables in the multivariate logistic regression. Besides time to EVT, we predefined coma and any hemorrhage (ICH and SAH) as the only covariables. Both were previously shown to be predictors of severity [25]. Because we expected a low absolute number of death cases, no multivariate analysis regarding mortality was conducted.





Comments (0)