ED physicians are accustomed to capnography in the settings of achieving return of spontaneous circulation in cardiopulmonary resuscitation, confirming placement of endotracheal intubation, and monitoring respiration during procedural sedation [16]. Routine capnography in non-intubated patients beyond these applications has been considerably more limited [22,23,24,25]. A possible explanation to the limited use is that capnography is available only on certain monitors such that they would not be considered or used elsewhere. Another issue is cost, although portable capnometers can now be purchased for less than $2,000. There is also limited evidence regarding waveform interpretation, as there are no diagnostic criteria as to what constitutes an abnormal capnogram or EtCO2. Therefore, it is unsurprising that capnography has not been explored as a screening test. Yet this brief measurement could be a missed opportunity for an earlier, as well as noninvasive, detection of pathophysiologic processes if its test characteristics prove clinically useful.
Our pilot data among intermediate-risk adult patients presenting to the ED represent the initial steps to determine if an accurate determination of a triage capnogram—comprising PECO2, EtCO2, and RR—can alert clinicians to acute processes or early decompensation. This study demonstrates that not only can RR be measured quickly and accurately, but also obtained along with PECO2 and EtCO2. Additionally, these results corroborate other studies showing that a low EtCO2 may indicate an underlying acidosis.
Patients with underlying pulmonary disease have documented average respiratory rates up to + 11 breaths/min greater than the average, healthy adult [26]. A precisely-measured, elevated RR by itself could signify greater minute ventilation and respiratory drive, and this can be further corroborated by an EtCO2 level. Yet the prevailing standard of care is to rely on an estimated RR, which was shown to be in wide disagreement with the actual RR, over a range of -10 and 14 breaths/min. The present study suggests that capnograms could significantly improve triage in this patient population.
Our results indicate that a low end-tidal CO2 (EtCO2 < 32 mmHg) could represent an underlying acidosis—with positive likelihood ratios of 4.68 (95% CI 2.59–8.45). Assuming a pre-test odds of 0.39 based on a 28% prevalence of acidemia, (\( o=\frac=\frac=0.39)\), the finding of EtCO2 < 32 mmHg has a post-test odds of (\( o=\left(0.39\right)\left(4.68\right)=1.83\)), which corresponds to a 65% post-test probability (\( p=\frac\times 100\%=65\%\)), roughly twice the pre-test probability. Unfortunately, the sensitivity 71.4% (95% CI 51.3-86.8) was also not sufficiently high enough to yield a negative likelihood ratio that is clinically useful to rule out acidemia. No study could be found in the literature among adult patients for comparison, but the utility of capnography has been more extensively investigated in pediatric patients. One study, for instance, demonstrated a correlation between EtCO2 < 31 mmHg and 96% specificity in detecting acidosis in cases of acute gastroenteritis [27]. This study of adult patients demonstrated that the specificity of acidosis was moderate, 84.7% (95% CI 74.3-92.1), indicating false positives that likely arose from increased respiratory drive secondary to pain [28]. Relatively poor correlation (R2 = 0.37) was found between EtCO2 and PvCO2 (Fig. 5). This has been observed in previous studies as well, and it is known that higher respiratory rates cause greater deviations [23].
The capnograms, while interpreted qualitatively, provide a rapid, visual perspective of the respiratory profile. The greater the steepness of the initial rise signifies better ventilation and perfusion (V/Q) matching; many pulmonary diseases have a slope with slower rise [29]. The next flat portion corresponds to the alveolar plateau, representing PECO2 arising from alveoli. A wider angle, steeper plateau indicates slower CO2 elimination and differential alveolar ventilation. This was observed in the capnogram (Supplemental Material, Fig. 2A) of a patient who presented with an opioid overdose. While alveolar hypoventilation is expected to increase EtCO2, the measured capnograms are qualitatively similar to that of normal, healthy patients. This is not unexpected as respiratory drive was likely restored almost completely by naloxone. Poor V/Q matching also manifests as a greater angle between the rise and plateau.
The absence of an of alveolar plateau in the mixed expired gas PECO2 (indicating rapid cycling) was found to be nearly always abnormal. The capnogram in Supplemental Material, Fig. 2A was highly unusual, including a rapid duty cycle, short alveolar plateau, PECO2 not returning to 0 mmHg, and respirophasic variations. In this particular case, the patient was experiencing a severe asthma exacerbation, with short breaths indicative of obstructive ventilatory process. A short duty cycle is not specific, however, as patients experiencing severe pain (Supplemental Material, Fig. 2B) will also be tachypneic. Finally, waveforms with low amplitudes were also indicative of EtCO2 < 32 mmHg.
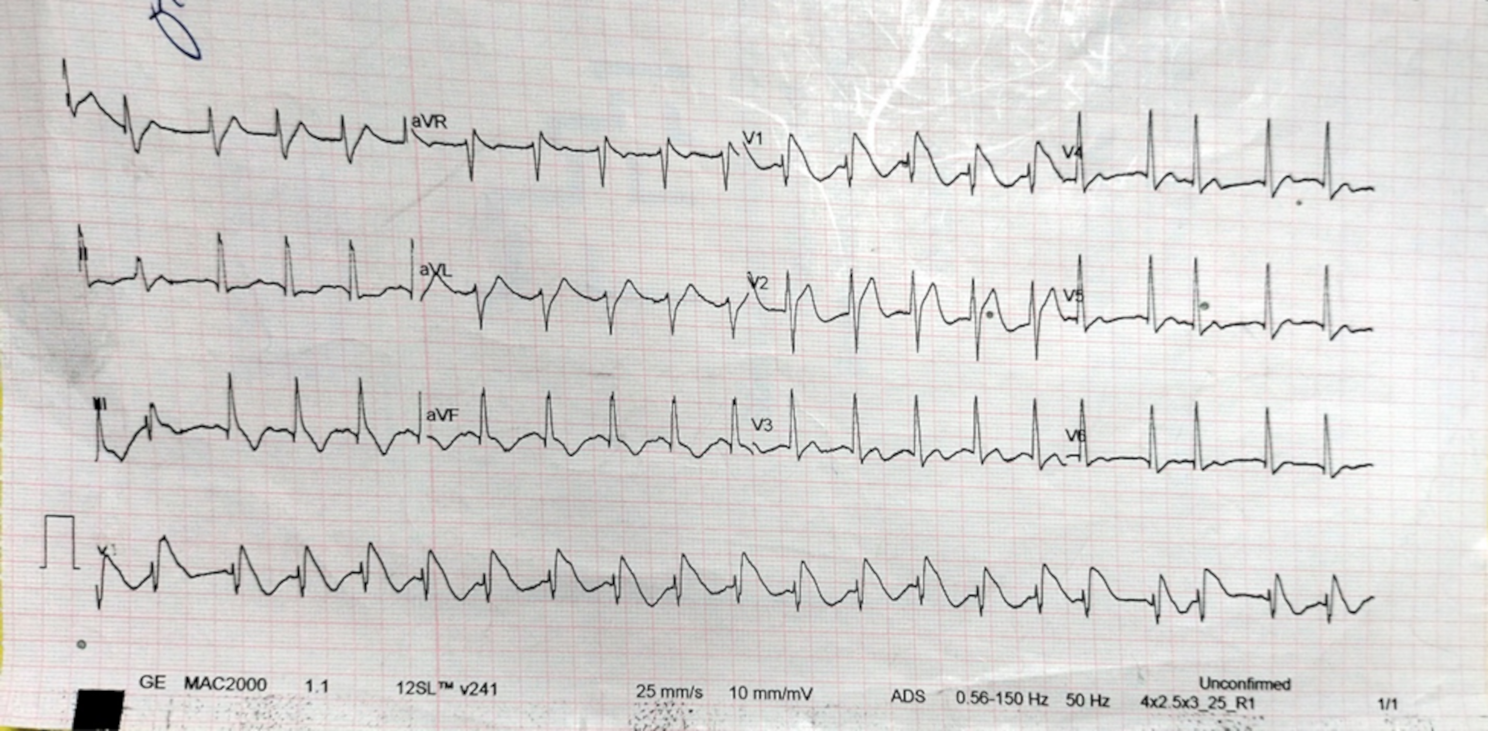
For true tachypnea (RR > 25), there is a positive likelihood ratio (LR+) of 2.14 (95% CI 1.05–4.39) of acidemia. If RR continues to be estimated, then it may be worthwhile to investigate the clinical impact of documenting rates as “slow”, “normal”, or “fast” instead, and to analyze the agreement with actual values. A continuation of this study would be to investigate the predictive value of triage EtCO2 on specific pathophysiologic processes, such as pneumonia or hypercapneic respiratory failure. It would also be interesting to study if merely a 10-second capnogram alone that was handed to a clinician like an electrocardiogram could lead to any significant changes in clinical management.






Comments (0)