
Remember me





Fasciitis ossificans is a pseudotumor of soft tissue, classified as a rare subtype of nodular fasciitis—a common reactive neoplasm of fibroblastic or myofibroblastic origin with an unknown etiology [1]. The presence of ossification in nodular fasciitis confirms the diagnosis of fasciitis ossificans. While it primarily affects adults without sex predilection, cases have been reported in children as well. Common locations include the extremities, head and neck, trunk, as well as the breast’s fascia or muscle. Due to its rapid growth, hypercellularity, and cytologic atypia, fasciitis ossificans is often mistaken for malignant sarcoma [2]. In some instances, it may be associated with medical conditions such as sarcoidosis or fibrodysplasia ossificans progressiva (FOP). Clinically, it typically presents as a growing asymptomatic mass, although tenderness, pain, or bleeding may occur. Surgical excision is considered curative, although recurrence can occur following incomplete excision.
While presentations at unusual sites have been described in case reports, to the best of the author’s knowledge, fasciitis ossificans of the penis has not been previously reported. Herein, we present the first documented case of a 73-year-old man presenting with fasciitis ossificans of the penis.
Case presentationA 73-year-old man presented at the outpatient clinic with sudden paraphimosis accompanied by a tumor measuring 2 × 2 cm arising from the glans penis, causing narrowing of the external urethral meatus and complaining about painful swelling of the penis persisting for the last two weeks. He noticed the tumor on the day of presentation, experiencing pain due to acute paraphimosis. A slightly and slow swelling of the entire penis had already commenced a couple of weeks prior to his visit, beginning the day after he underwent a rigid cystoscopy at a urology practice. During this cystoscopy, the patient experienced sudden severe pain and subsequently suffered from gross hematuria. In the following days, the swelling of the penis increased and then stabilized, while the hematuria ceased the day after the traumatic cystoscopy. The patient noticed swelling at that time but no further increase until about two weeks before the consultation in the outpatient clinic. He avoided consultation at the urological practice, where the cystoscopy was performed. The urologist there noted from his cystoscopy only a stenotic external urethral meatus without further findings. The patient had reported him urinary difficulties without pain or hematuria for several weeks before seeking urological consultation. Approximately six months prior to this visit, a routine check-up had been conducted without any abnormalities. His medical history included lower urinary tract symptoms attributed to mild benign prostatic hyperplasia (BPH) and “non-insulin-dependent diabetes mellitus”, for which he did not require treatment.
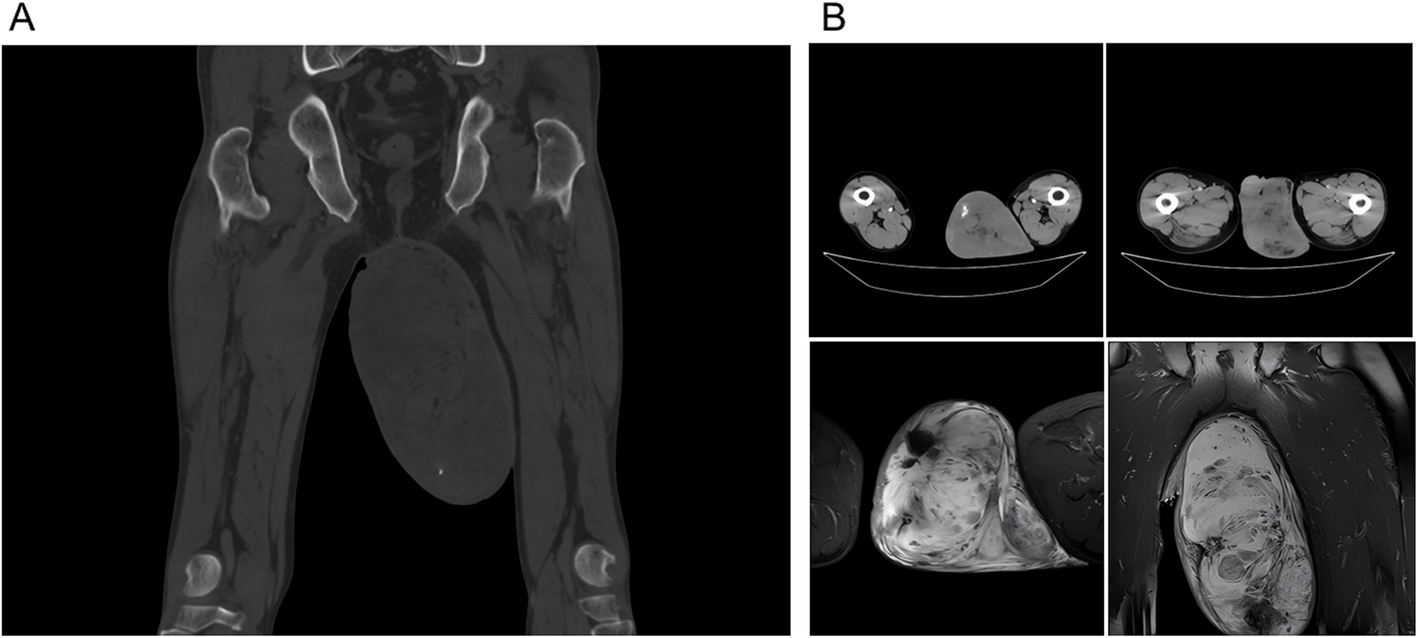
Upon initial presentation at our outpatient clinic, paraphimosis was promptly relieved. Due to suspicion of urethral carcinoma, a biopsy of the tumor was performed. The initial histopathological analysis did not yield definitive results. P-16 analysis was negative, and AE 1/AE 3 stains were not detected. Signs of ossification were already observed. With a provisional diagnosis of “papillary urethritis with metaplastic ossification with high-grade squamous dysplasia—consistent with carcinoma in situ”, the sample was sent for a second opinion. However, this analysis also failed to provide conclusive results due to a high amount of necrotic tissue. Subsequently, MRI imaging was performed, revealing an expansive process in the distal part of the corpus spongiosum measuring 3.8 × 1.9 cm in diameter, with a low apparent diffusion coefficient (ADC) signal alteration and significant contrast media enhancement (Fig. 1). There were no indications of lymph node involvement. After obtaining informed consent from the patient, a partial penile amputation was performed due to suspected penile carcinoma.
Fig. 1
MRI of the tumor formation with size indication
Histological examination of the specimen revealed further staining characteristics: desmin negative, smooth muscle actin positive, slightly positive antigen expression of CD10, and CD34 marking vessels. The tumor originated from the glans penis and extended to the urethra without mucosal breach. Mitotic activity was rare and confined to the basal cell layer without p63 hyperexpression, and the Ki-67 proliferation index was low at 10%. Centrally, the tumor exhibited clear signs of ossification, characterized by abundant osteoid, osteoblasts, and osteoclasts (see Figs. 2 and 3). There were no indications of squamous cell carcinoma. Since the mass on the penis was misinterpreted as penile carcinoma at the initial presentation, no photographic documentation was performed.
Fig. 2
Top left: mineralized bone. Down right: osteoid; magnification 20x; HE (Hematoxylineosin)-staining
Fig. 3
Mineralized bone beside osteoid; magnification 20x; HE (Hematoxylineosin)-staining
Comments (0)