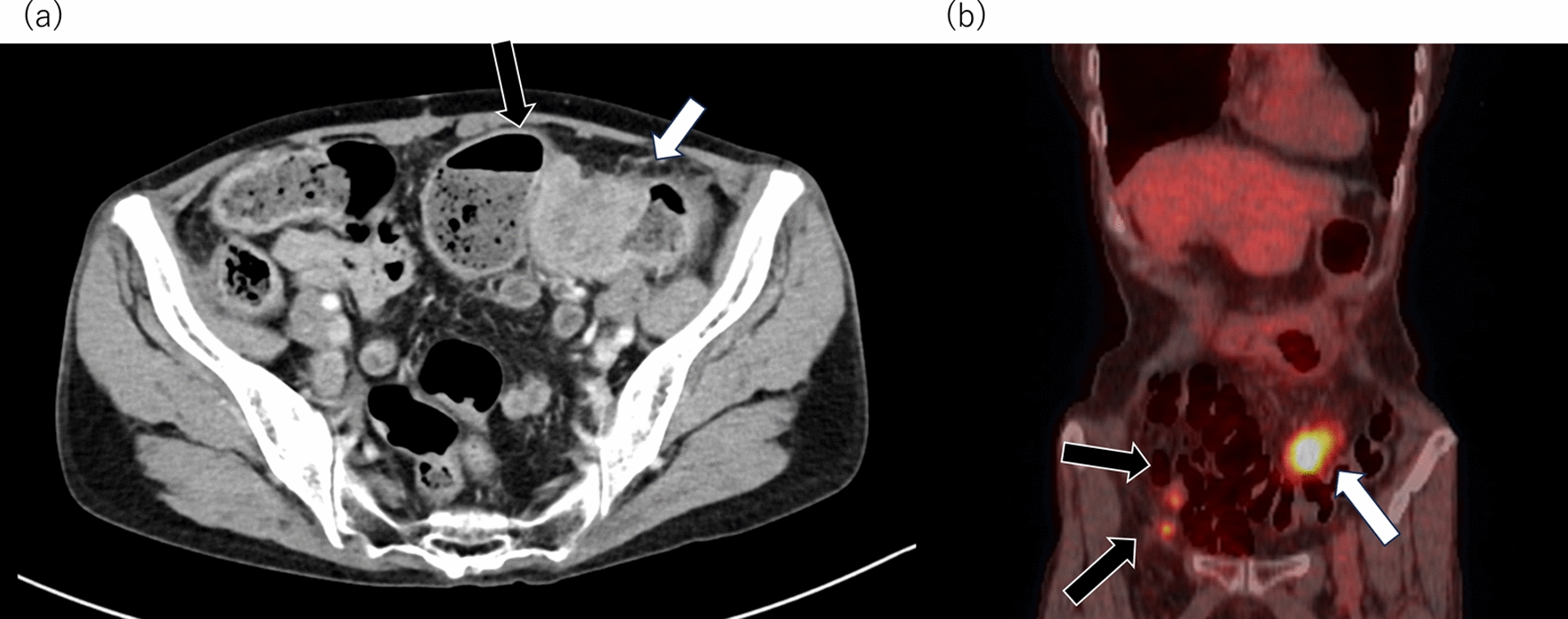
Pylephlebitis, which is defined as infective thrombophlebitis of the portal vein, is relatively uncommon. The mortality remains notably high in the contemporary era despite advancements in antibiotic therapy and surgical interventions [1,2,3]. This condition typically manifests secondary to uncontrolled infections within regions drained by the portal and mesenteric venous systems [5]. Appendicitis and diverticulitis are the predominant causative factors [6,7,8]. Other underlying causes include cholecystitis, pancreatitis, malignancies, and infections localized within the abdominal and pelvic areas [9,10,11,12,13]. Specifically, in cases of appendicitis and diverticulitis, the combination of inflammation propagation from bacterial invasion, originating in the peripheral mesenteric veins and extending to the central portal vein, with a reduction in circulatory volume due to fever and dehydration, and an escalation in blood viscosity collectively contributes to septic thrombus formation within the portal vein [14]. The likelihood of developing septic portal vein thrombosis is significantly increased, particularly in cases of concomitant disseminated intravascular coagulation due to sepsis [15] (Fig. 5).
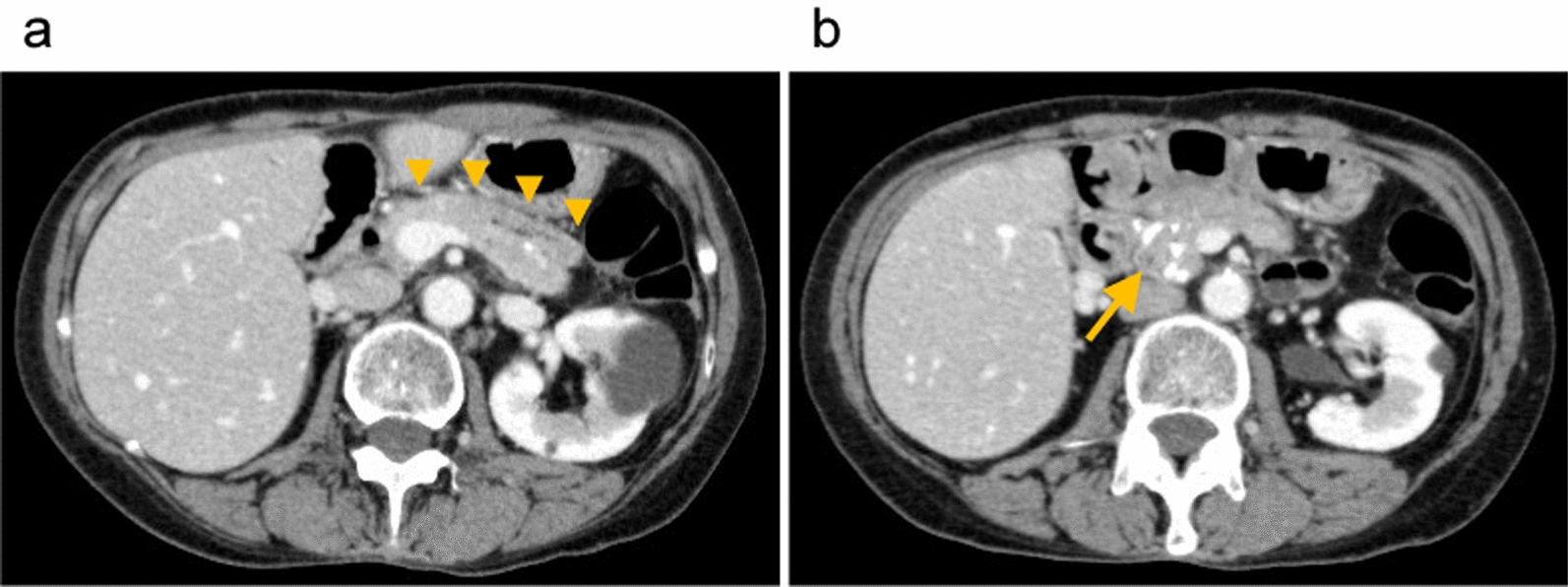
The diagnosis of pylephlebitis requires the confirmation of portal mesenteric vein thrombosis and bacteremia. Owing to the invasive nature of the procedures, proof of infectious portal thrombosis is seldom available. Thus, clinical presentation, radiographic findings, and cultures lead to the diagnosis [9, 16]. Clinical symptoms, including fatigue, fever, abdominal discomfort, nausea, vomiting, diarrhea, and anorexia, often manifest nonspecifically. Advanced symptoms include hepatomegaly and jaundice. Therefore, imaging studies that identify thromboses in the portal system are valuable diagnostic alternatives. Portal-phase imaging is favored in the acute phase not only because of its accessibility and the high-quality clinical data it provides but also because of its capability to discern complications, such as hepatic abscesses or intestinal ischemia [6, 17]. Nonetheless, early diagnosis can be elusive owing to nonspecific symptomatology. In this case, the condition was identified as more severe.
The therapeutic strategy for this condition involves three main steps: eradication of the causative pathogens, removal of infectious thrombi, and definitive management of the primary source of infection [16, 18]. However, there are no standardized treatment protocols. Current management approaches typically employ a combination of antibiotic therapy, surgical intervention, and anticoagulation, underscoring the need for prompt and appropriate intervention.
Antibiotic treatment consists of broad-spectrum antibiotics, with the choice of empiric antibiotics depending on the most probable source of infection and the most likely involved organisms, regardless of bacteriaemia [16]. When blood cultures yield positive results, treatments are tailored to target the identified pathogens. Blood cultures are advised for patients with suspected thrombotic portal vein phlebitis, as suggested in a previous study. However, blood cultures were positive at a previously reported rate of 42–62% [7, 9, 19].
Pylephlebitis is often a polymicrobial infection caused by gram-negative, gram-positive, aerobic, and anaerobic bacteria, especially E. coli, Streptococcus species Pluralis (spp.), and Bacteroides spp. According to previous reports, antibiotics were administered in almost all patients (94.6–100%) [7, 9, 19, 20]. In the present case, B. fragilis was isolated from both the blood and the intra-abdominal abscesses. B. fragilis is an obligate anaerobe that plays a pivotal role in the gut microbiota [21]. The recommended drugs for the empirical treatment of B. fragilis infections are active against aerobic bacteria, including fecal flora. Thus, the primary therapeutic choice is MNZ or piperacillin/tazobactam (PIPC/TAZ). Secondary options include carbapenems such as MEPM [22].
A noteworthy feature of this case was the multidrug-resistant nature of B. fragilis, which considerably impacted the antibiotic selection. Although resistance to MNZ, PIPC/TAZ, and carbapenems was once deemed exceedingly rare, recent global reports have suggested an increasing trend in the resistance of B. fragilis isolates to carbapenem antibiotics [23,24,25,26]. However, currently, in Japan, B. fragilis resistance to carbapenems is still rare (approximately 2%) [27,28,29]. In addition, carbapenem-resistant B. fragilis strains often exhibit an increased propensity to develop resistance to other anaerobic antibiotics, rendering them multidrug-resistant. The cfiA gene is specific to B. fragilis, encoding the carbapenem-hydrolyzing metallo-β-lactamase, and is expressed in 2–7% of the strains. The presence of the cfiA gene alone does not invariably confer carbapenem resistance; it has been postulated that an insertion sequence in the promoter region upstream of the cfiA gene might be responsible for pronounced carbapenem resistance [28, 30, 31]. In this case, the primary determinant for acquiring an infection caused by a multidrug-resistant strain is attributed to the patient's origin in China. In addition, using MALDI–TOF mass spectrometry for protein spectral analysis allowed for differentiation between cfiA gene-positive and gene-negative strains almost simultaneously with bacterial identification. Consequently, an antibiotic regimen centered on MNZ was promptly initiated.
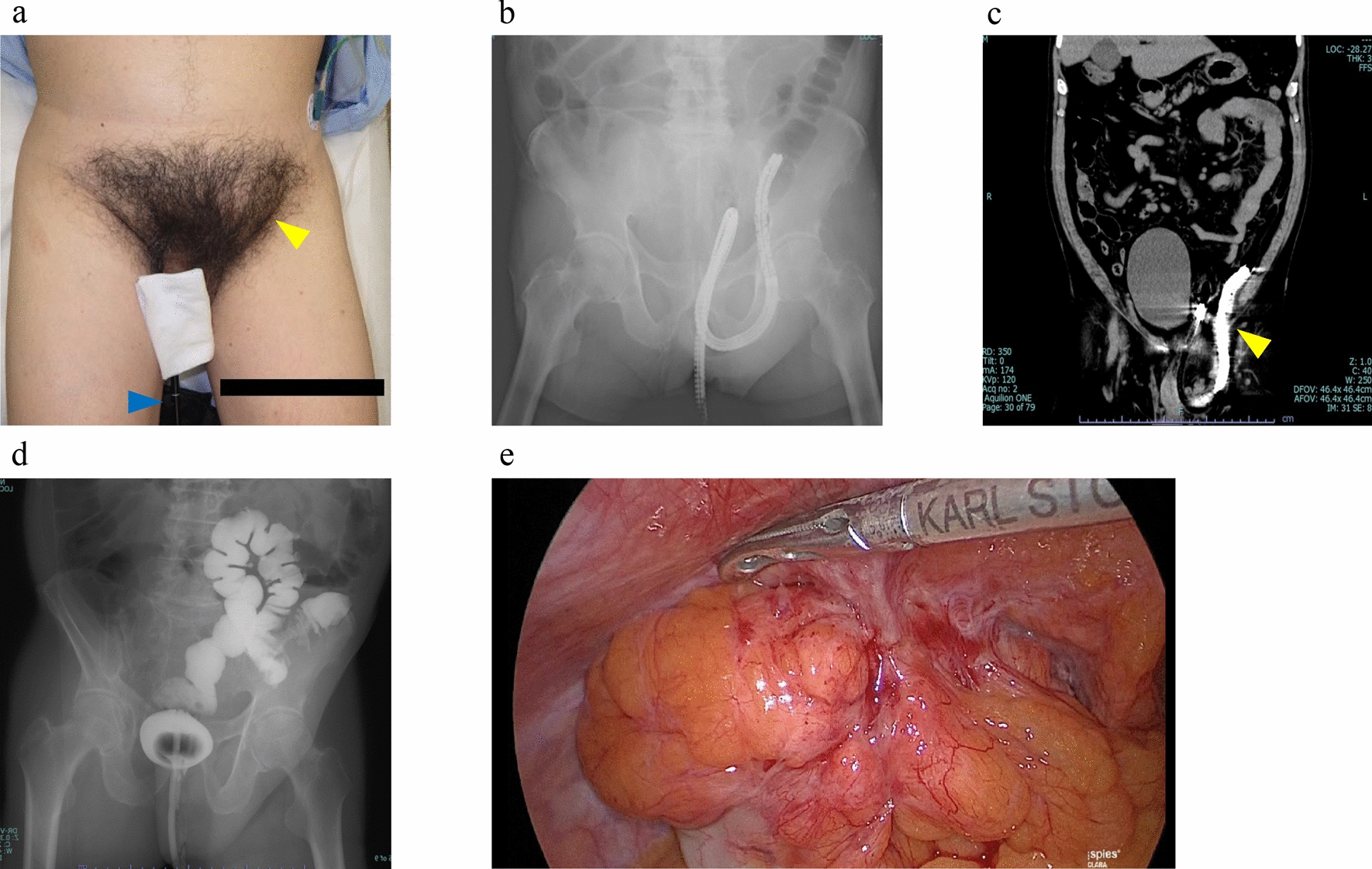
Invasive therapeutic additions, such as the removal of the primary infection site or drainage of intra-abdominal abscesses via surgical or radiologically guided percutaneous approaches, are sometimes essential and effective in controlling the infection source. This case showed that management of the infection was challenging despite early identification of the causative bacteria, antibiotic susceptibility, and prompt antibiotic intervention. The appendectomy was deemed a critical component of the surgical treatment strategy. Nevertheless, owing to severe obesity and extensive involvement of abscess cavities during the procedure, the identification and excision of the appendix were deemed unfeasible. Therefore, we opted for surgical lavage drainage via laparotomy. OAM is also believed to yield the best outcomes. Generally, the objectives of OAM include prevention of increased intra-abdominal pressure, a straightforward approach to subsequent surgeries or lavages, and proliferation of abdominal infections [32, 33]. Using devices for provisional closure, OAM is sustained until control over bleeding, intra-abdominal contamination, and decreased intra-abdominal pressure was achieved, allowing for safe closure. The ability to effortlessly access and perform lavage of the abdominal cavity, even within the confines of an intensive care unit, has proven to be of immense value.
The role of anticoagulation therapy in the treatment of thrombophlebitis remains ambiguous owing to the infrequency of the condition and insufficient evidence. Thus, its implementation should be considered on a case basis. Situations warranting consideration for anticoagulant initiation include extensive thrombosis in the mesenteric vein, observed thrombus progression tendencies, persistent bacteremia despite antibiotic administration, or the presence of hypercoagulable states [20, 34]. This case demonstrated that anticoagulation therapy using heparin and edoxaban resulted in the resolution of the portal vein thrombus. After assessing the risk of hemorrhage and the potential worsening of portal vein thrombosis, we proceeded with surgical drainage, maintained anticoagulation therapy for portal vein thrombosis, and acknowledged the intrinsic bleeding risk. As a result, the diminution of the portal vein thrombus facilitates hemorrhage control from the collateral pathways, enabling secure abdominal closure.





Comments (0)