
Remember me








Breast cancer is the most common malignancy in women in the United States and is the second leading cause of death from cancer after lung cancer.[1] Better elucidation of breast cancer heterogeneity has allowed the development of more effective individualized therapeutic approaches.[2] The high incidence of breast cancer and the complex mechanisms in its pathogenesis necessitate better elucidation of the molecular features of breast cancer. In the last few years, significant progress has been made in the discovery of new drugs for the treatment of this malignancy.
Fibroblast growth factors (FGFs) comprise 22 members and are involved in various physiological processes such as embryogenesis, angiogenesis, and tissue homeostasis by activating tyrosine kinase FGF receptors (FGFRs) (FGFR1, FGFR2, FGFR3, and FGFR4) and by initiating intracellular signaling pathways, including the RaS-MAPK and PI3K/AKT pathways.[3] FGFs contribute to the maintenance of pluripotency and self-renewal of stem cells in both normal and tumor tissue.[4] FGFs are classified as canonical hormone-like (canonical autocrine, paracrine endocrine) FGFs and intracellular FGFs. Fibroblast growth factor 11 (FGF11) is one of the intracellular FGFs and functions intracellularly independently of the FGF receptor.[5] Canonical hormone-like FGFs are secreted and signal by binding to FGFRs with heparan sulfate proteoglycans or klotho proteins.[6] Intracellular FGFs (FGF11–FGF14) have a nonsecreted nuclear localization signal.[7]
Abnormal FGF/FGFR activation (genetic modifications or overexpression) have been associated with abnormal cell proliferation, tumor formation and progression in various tumor types such as breast, lung, stomach, bladder, and hematological malignancies.[8–12] There are few studies investigating FGF/FGFR activation in breast cancer. In a study, FGF or FGFR aberrations were detected in 32.1% of breast cancer patients.[13]
The prognostic role of FGF11 has only been reported in cancers such as nasopharyngeal carcinoma[14] and prostate cancer.[15] It has been reported that the copy number of the FGF11 gene is associated with the risk of lung cancer in heavy smokers.[16] In this study, it was aimed to compare the FGF11 expression levels in hormone receptor (HR)-positive, human epidermal reseptor-2 (HER2)-negative breast tumor tissue and healthy breast tissue, and investigate the effect of the FGF11 expression on survival in HR-positive HER2-negative breast cancer patients.
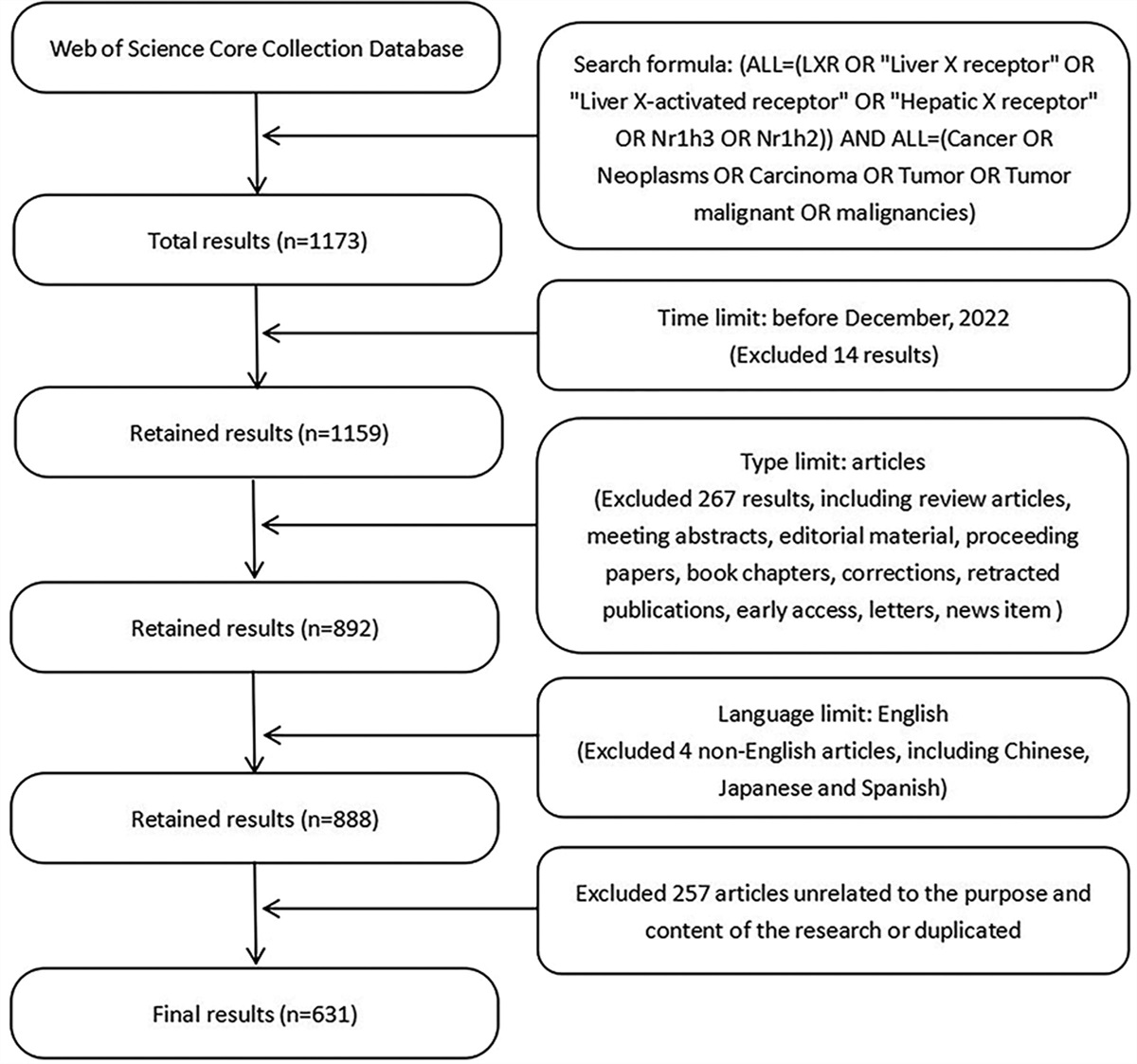
2. Materials and methodsPatients diagnosed with de novo metastatic HR-positive, HER2-negative breast cancer, who were followed-up in the medical oncology clinics of Ankara Numune Training and Research Hospital and Ankara Bilkent City Hospital, between January 2013 and June 2023, were included in this study. The patient’ files in the pathology hospital archive were retrospectively scanned. Age, sex, breast cancer family history, Eastern Cooperative Oncology Group Performance Status, pathological staining characteristics of the tumor, metastatic sites, number of metastases, and treatments received by the patients were recorded from the patients’ files. Additionally, breast biopsy paraffin blocks of healthy individuals who underwent breast biopsy due to benign lesions in the pathology department of Ankara Bilkent City Hospital were used.
To determine the FGF11 expression rate, breast tumor tissue of metastatic, HR-positive, HER2-negative breast cancer patients diagnosed by breast biopsy and healthy breast tissue of healthy individuals who underwent breast biopsy due to benign lesions were used.
Overall survival (OS) was defined as the time interval from the time of onset of metastatic disease to death due to any reason or last follow-up. Progression-free survival (PFS) was defined as the time interval from initiation of the treatment to progression or death from any cause. The data obtained were analyzed.
The study was approved by the Ankara City Hospital Ethics Committee with decision number E1/2307/2022 in compliance with the Helsinki Declaration.
2.1. FGF11 immunohistochemical (IHC) staining and staining evaluationThe ICH method allows the identification of highly specific proteins in tissue sections. The method we used is the IHC identification of FGF11 in appropriate formalin-fixed paraffin-embedded tissues. Ten percent of formalin-fixed tissues waited for 24 hours, tissues processed in Leica ASP300S Fully Enclosed Vacuum Tissue Processor and embedded in Leica EG1150 C Cold Plate for Modular Tissue Embedding System then sections were cut into 3 µm thick from paraffin blocks obtained from breast tumor tissue and healthy breast tissue on Leica RM2125RT Rotary Microtome. After these processed sections put in the instrument for immunohistochemical staining, baked deparaffinization and incubation were performed in a BOND-MAX Fully Automated IHC and ISH Staining System. Heat-induced EDTA antigen retrieval (pH 9) for 20 minutes hidrojen peroksite 10 minutes, marker FGF antibody (anti-FGF11 [MM0282-6J20] [ab89713] mouse monoclonal, Abcam Inc., Waltham, MA) and incubated for 200 minutes at a dilution of 1:100. As the secondary elements, a Leica HRP conjugated polymer detection kit was used (DS9800, New Castle, United Kingdom), postpolymer for 8 minutes, polymer for 8 minutes, DAB for 8 minutes, and hematoxylene for 10 minutes, washed with washing solution at each step, dehydrated and covered with Entellan.
For FGF11, scoring was done according to the staining rate in the breast tumor tissue and healthy breast tissue pathology blocks. For the scoring, 0% to 5% was classified as score 0, 6% to 10% was classified as score 1, 11% to 50% was classified as score 2, and 51% to 100% was classified as score 3.[14] Placenta was used as a positive control.
2.2. Statistical analysisStatistical analyses were performed using IBM SPSS Statistics for Windows 25.0 (IBM Corp., Armonk, NY). Descriptive statistics were presented as the number (n) and percent (%) for the categorical variables and as the median (min–max) for the continuous variables. The Kaplan–Meier method was used to compare the survival and PFS times between various clinical parameter groups. The Fisher exact test and Mann–Whitney U test were used to compare the categorical variables. P < .05 was considered statistically significant.
3. ResultsA total of 62 participants were included in the study, including 38 breast cancer patients and 24 healthy controls. The mean follow-up period of the patients was 31.37 ± 19.25 months. The median age of the patient group was 62.50 (35–78) years, and the median age of the healthy control group was 61.34 (38–77) years. There was no difference in the median age between the groups. In the patient group, 9 patients (23.7%) had a family history of breast cancer. The Eastern Cooperative Oncology Group Performance Status was 0 in 11 patients (28.9%), 1 in 16 (42.1%) patients, 2 in 9 (23.7%) patients, and 3 in 2 (5.3%) patients (Table 1).
Table 1 - Sociodemographic and clinical characteristics in the groups. Variables Patient group, N = 38 Healthy control group, N = 24 P-value Age, median (min–max) 62.50 (35–78) 61.34 (38–77) .07 Family history of breast cancer, n (%) No 29 (76.3) Yes 9 (23.7) ECOG PS, n (%) 0 11 (28.9) 1 16 (42.1) 2 9 (23.7) 3 2 (5.3) ER, n (%) 11%–89% 15 (39.5) ≥90% 23 (60.5) PR, n (%) 1%–10% 6 (15.8) 11%–89% 25 (65.8) ≥90% 7 (18.4) HER2 score, n (%) Score 0 27 (71.1) Score 1 3 (7.9) Score 2/FISH negative 8 (21.1) Grade, n (%) 1 12 (31.6) 2 20 (52.6) 3 6 (15.8) Ki67, n (%) <20% 15 (40.5) ≥20% 17 (46) Unknown 5 (13.5) Bone metastasis, n (%) No 6 (15.8) Yes 32 (84.2) Liver metastasis, n (%) No 29 (76.3) Yes 9 (23.7) Lung metastasis, n (%) No 27 (71.1) Yes 11 (28.9) Surrenal metastasis, n (%) No 34 (89.5) Yes 4 (10.5) Nonregional lymph node metastasis, n (%) No 28 (73.7) Yes 10 (26.3) Bone marrow metastasis, n (%) No 37 (97.4) Yes 1 (2.6) Ovarian metastasis, n (%) No 36 (94.7) Yes 2 (5.3) Peritoneal metastasis, n (%) No 37 (97.4) Yes 1 (2.6) First-line treatment, n (%) Chemotherapy 5 (13.2) Hormonal therapy 15 (39.5) CDK4/6 inhibitor + aromatase inhibitör 18 (47.4) Palliative radiotherapy, n (%) No 21 (55.3) Yes 17 (44.7) Treatment response, n (%) Partial response 11 (28.9) Stable response 22 (57.9) Progressive disease 5 (13.2) Second-line treatment, n (%) No 24 (63.2) Yes 14 (36.8) Disease progression, n (%) No 14 (36.8) Yes 24 (63.2) Mortality, n (%) Alive 17 (44.7) Exitus 21 (55.3)Mann–Whitney U test, P < .05 is statistically significant; ECOG PS = Eastern Cooperative Oncology Group Performance Status, ER = estrogen receptor, FISH = fluorescent in situ hybridization, HER2 = human epidermal reseptor-2, PR = progesterone receptor.
The estrogen receptor (ER) level was 11% to 89% in 15 (39.5%) patients and ≥ 90% in 23 (60.5%) patients. The progesterone receptor level was 1% to 10% in 6 (15.8%) patients, 11% to 89% in 25 (65.8%) patients, and ≥ 90% in 7 (18.4%) patients. The HER2 score was 0 in 27 (71.1%) patients, 1 in 3 (7.9%) patients, 2 and the fluorescent in situ hybridization (FISH) test was negative in 8 (21.1%) patients. From the pathological staining characteristics, it was determined that 12 (31.6%) patients were grade 1, 20 (52.6%) were grade 2, and 6 (15.8%) were grade 3. The Ki67 level was < 20% in 15 (40.5%) patients, ≥20% in 17 (46%) patients, and unknown in 5 (13.5%) patients (Table 1).
Bone metastasis was found in 32 (84.2%) patients, liver metastasis in 9 (23.7%) patients, lung metastasis in 11 (28.9%) patients, adrenal metastasis in 4 (10.5%) patients, nonregional lymph node metastasis in 10 (26.3%) patients, bone marrow metastasis in 1 (2.6%) patient, ovarian metastasis in 2 (5.3%) patients, and peritoneal metastasis in 1 (2.6%) patient (Table 1).
As metastatic first-line treatment, 5 (13.2%) patients received chemotherapy due to visceral crisis, 15 (39.5%) received hormonal therapy (tamoxifen or aromatase inhibitor), and 18 (47.4%) received CDK4/6 inhibitor + aromatase inhibitor. Moreover, 17 (44.7%) patients received palliative bone radiotherapy. There was disease progression in 24 (63.2) patients under metastatic first-line treatment, and 28 (73.7%) patients were able to receive second-line treatment. At the data-cut date, 17 (44.7%) patients were alive, and 21 (55.3%) patients had expired (Table 1).
The FGF11 staining features are shown in Figure 1. There was a significant difference in the FGF11 expression levels between the patient group and the healthy control group (P = .002). The number of patients with a FGF11 expression level score of 0 was significantly higher in the healthy control group compared to the patient group (75% vs 34.2%). The number of patients with a FGF11 expression level score of 1 (15.8% vs 12.5%) and score of 2 (18.4% vs 12.5%) was significantly higher in the patient group compared to the healthy control group. Moreover, while none of the patients in the healthy control group had a FGF11 expression level score of 3, 12 of those (31.6%) in the patient group had FGF11 expression level score of 3 (Table 2).
Table 2 - Comparison of FGF11 levels between groups. Variables Whole group, N = 62 Healthy control group, N = 24 Patient group, N = 38 P-value FGF11, n (%) Score 0 (0%–5%) 31 (50.0) 18 (75.0) 13 (34.2) .002 Score 1 (6%–10%) 9 (14.5) 3 (12.5) 6 (15.8) Score 2 (11%–50%) 10 (16.1) 3 (12.5) 7 (18.4) Score 3 (51%–100%) 12 (19.4) 0 (0.0) 12 (31.6)Fisher’s exact test, P < .05 is statistically significant; FGF11 = fibroblast growth factor 11.
 Figure 1.:
Figure 1.: FGF11 immunohistochemical staining and scoring. (A) Placenta positive control, (B) FGF11 score 0, (C) FGF11 score 1, (D) FGF11 score 2, (E) FGF11 score 3, and (F) hematoxylin eosin staining of FGF11 score 3 paraffin block. FGF11 = fibroblast growth factor 11.
There was no difference in the FGF11 levels according to the ER, progesterone receptor, HER2, grade, and Ki67 levels or presence of bone, liver, lung, adrenal, and nonregional lymph node metastasis, or number of metastatic sites (Table 3).
Table 3 - Comparison of FGF11 levels according to the clinical characteristics of the patient group. Variables FGF11 P-value Score 0 (0%–5%) Score 1 (6%–10%) Score 2 (11%–50%) Score 3 (51%–100%) ER, n (%) <90% 6 (46.2) 3 (50) 3 (42.9) 3 (25) .665 ≥90% 7 (53.8) 3 (50) 4 (57.1) 9 (75) PR, n (%) <90% 8 (72.7) 4 (80) 5 (83.3) 8 (80) 1.000 ≥90% 3 (27.3) 1 (20) 1 (16.7) 2 (20) HER2 score, n (%) Score 0/1 9 (69.2) 5 (83.3) 6 (85.7) 10 (83.3) .853 Score 2/FISH negative 4 (30.8) 1 (16.7) 1 (14.3) 2 (16.7) Grade, n (%) 1 4 (30.8) 3 (50) 2 (28.6) 3 (25) .404 2 8 (61.5) 1 (16.7) 3 (42.9) 8 (66.7) 3 1 (7.7) 2 (33.3) 2 (28.6) 1 (8.3) Ki67, n (%) <20% 6 (54.5) 0 (0) 2 (33.3) 7 (58.3) .359 ≥20% 5 (45.5) 3 (100) 4 (66.7) 5 (41.7) Bone metastasis, n (%) No 2 (15.4) 2 (33.3) 1 (14.3) 1 (8.3) .535 Yes 11 (84.6) 4 (66.7) 6 (85.7) 11 (91.7) Liver metastasis, n (%) No 11 (84.6) 5 (83.3) 6 (85.7) 7 (58.3) .486 Yes 2 (15.4) 1 (16.7) 1 (14.3) 5 (41.7) Lung metastasis, n (%) No 6 (46.2) 5 (83.3) 6 (85.7) 10 (83.3) .146 Yes 7 (53.8) 1 (16.7) 1 (14.3) 2 (16.7) Surrenal metastasis, n (%) No 10 (76.9) 6 (100) 6 (85.7) 12 (100) .282 Yes 3 (23.1) 0 (0) 1 (14.3) 0 (0) Nonregional lymph node metastasis, n (%) No 10 (76.9) 4 (66.7) 5 (71.4) 9 (75) 1.000 Yes 3 (23.1) 2 (33.3) 2 (28.6) 3 (25) Number of metastasis sites, n (%) <5 7 (53.8) 2 (33.3) 4 (57.1) 7 (58.3) .836 ≥5 6 (46.2) 4 (66.7) 3 (42.9) 5 (41.7)Fisher’s exact test, P < .05 statistically significant; ER = estrogen receptor, HER2 = human epidermal reseptor-2, PR = progesterone receptor, FISH = fluorescent in situ hybridization.
The median OS in the patient group was 45.46 (26.54–64.39) months (Fig. 2A), while the 2-year OS was 70.3% and 5-year OS was 26.3%. In the subgroup analysis performed according to the FGF11 scoring in the patient group, the median OS was similar between the groups (P = .297) (Fig. 2B). However, numerically, the median OS was higher in the group with a FGF11 score of 0 to 1 (46.50 [28.45–64.54]) than in the group with a FGF11 score of 2 (17.46 [8.57–26.36]) and FGF11 score of 3 (28.86 [7.65–32.45]).
 Figure 2.:
Figure 2.: OS and PFS results of the patient group. (A) OS of the patient group, (B) comparison of OS of the patient group according to FGF11 levels, (C) PFS of the patient group, and (D) comparison of PFS of the patient group according to FGF11 levels. FGF11 = fibroblast growth factor 11, OS = overall survival, PFS = progression-free survival.
The median PFS in the patient group was 22.00 (13.70–30.29) months (Fig. 2C), while the 2-year PFS was 45.8% and 5-year PFS was 27.5%. In the subgroup analysis performed according to the FGF11 scoring in the patient group, median PFS was similar between the groups (P = .377) (Fig. 2D). However, numerically, the median PFS was higher in the group with a FGF11 score of 0 to 1 (23.83 [10.2–50.45]) than in the group with a FGF11 score of 2 (13.50 [7.59–19.40]) and FGF11 score 3 (22.00 [8.36–35.63]).
4. DiscussionTo the best of our knowledge, this is the first study in the literature investigating FGF11 expression levels and it was detected that the FGF11 expression level was higher in HR-positive, HER2-negative breast tumor tissue compared to healthy breast tissue, which suggests that it may be a predictive marker for breast cancer formation. There are a limited number of studies in the literature investigating FGF/FGFR abnormalities in breast cancer. FGF overexpression has been shown to increase estrogen-independent cell proliferation and metastatic formation in HR-positive breast cancer.[17] The amplification of FGFR1 is the most common FGF abnormality in breast cancer and it is amplified in approximately 15% of HR-positive breast cancer and approximately 5% of triple-negative breast cancer.[18] FGFR2 amplification occurs in approximately 1% of breast cancers and 4% in triple-negative breast cancer.[19,20] In another study, FGFR3 amplification was detected in 0.5% and FGFR4 amplification was 2.3% to 10% in breast cancer.[19,21]
Additionally, it was detected that in the HR-positive, HER2-negative breast cancer patients herein, the median OS and PFS were numerically better in the group with FGF11 expression score of 0 to 1 than the group with a FGF11 expression score of 2 and 3. But this difference did not reach statistical significance. No studies could be found in the literature examining the effect of FGF11 on survival in breast cancer. A few studies were encountered that investigated breast cancer survival with other FGFR abnormalities. In one study, patients with a high FGFR1 expression or increased copy number exhibited lower OS rates compared to the remaining patient group.[22] Another study showed that OS and disease-free survival decreased as the FGFR2 levels increased.[23] However, the fact that FGFR2 increase can also be seen in healthy breast tissue has reduced the possibility of FGFR2 being a targetable therapy.[24] The presence of the FGFR4-R388 allele has been associated with increased lymph node metastasis and decreased survival.[25] In the current study, numerically better OS and PFS results were obtained in the group with a FGF11 score of 0 to 1, although it did not reach statistical significance, which may have been due to the small number of patients.
The numerically better OS and PFS detection in the group with low aFGF11 expression suggests endocrine resistance that may develop with increased FGF11 expression, because endocrine therapies are mostly preferred in first-line treatment in this patient group. There are some studies that have investigated the relationship between FGF/FGFR abnormalities and endocrine resistance. Cancer-associated fibroblasts (CAFs), which are considered to be the source of FGF ligands, are densely present in the tumor stroma and stimulate cancer cell proliferation, migration, invasion, and angiogenesis.[26] CAFs may lead to endocrine resistance by affecting the FGF/FGFR system. FGF7 secreted by CAFs interacts with FGFR2 and stimulates proteasomal degradation after ER phosphorylation, making breast cancer cells resistant to endocrine therapy.[27] FGFR1 amplification has been shown to correlate with aberrant signaling (ligand dependent and ligand independent) and this may lead to resistance to endocrine therapies in breast cancer.[24,25] Furthermore, FGFR1 amplification and overexpression have been associated with resistance to combined endocrine therapy with CDK4/6 inhibitors in in vitro or in vivo studies.[28] One study found that the FGFR3 expression was higher in the tamoxifen-insensitive subgroup of HR-positive breast cancer patients.[29] In a retrospective analysis, an increased FGFR4 level was shown to be associated with a response to tamosifen and survival in ER-positive patients.[30]
The predictive and prognostic effect of FGF/FGFR abnormalities in other solid tumors other than breast cancer has been investigated. In a study examining the relationship between FGF11 levels and survival in patients with human papillomavirus positive oropharyngeal squamous cell carcinoma, it was found that increased FGF11 levels were associated with poor OS and disease-specific survival.[31] In prostate cancer, the androgen receptor has been shown to work to suppress metastasis[32] and FGF11 enables prostate cancer cell invasion through FGF11/miRNA-541/AR/MMP9 signaling.[15] In a study conducted in patients diagnosed with nonsmall cell lung cancer, it was shown that the FGF11 expression in the tumor tissue of these patients was higher than in healthy tissue, and an increased FGF11 level was associated with poor OS.[33] FGF11 is known to increase hypoxia inducible factor 1-alpha (HIF-1α) expression, which is a transcriptional regulator of the hypoxia signaling pathway, and it appears impaired in cancer progression.[34] On the contrary, the oncogenic effect of FGF11 decreases with the destruction of HIF-1α in nonsmall cell lung cancer.[33] HIF-1α has been found to be overexpressed in ductal carcinoma in situ and early stage breast cancer, and increased HIF-1α level correlates with tumor grade and invasion.[35
Comments (0)