
Remember me








Acute ischemic stroke (AIS) refers to the softening and necrosis of local brain tissue due to blood circulation disorders, ischemia, and hypoxia. Over the past 30 years, 80% of developing countries have witnessed a shift in disease patterns from infectious to non-communicable, with stroke emerging as one of the most prevalent debilitating conditions. Current global stroke statistics reveal that stroke remains the second-leading cause of death and the third-leading cause of mortality and disability worldwide. Ischemic stroke (IS), comprising 70% of all strokes, is associated with a high risk of long-term and recurrence occurrences.[1,2] AIS is characterized by elevated disability and mortality rates, posing a significant threat to public health and increasing the economic burden on families and society.
Currently, confirmed effective treatments for early recanalization in AIS primarily encompass intravenous thrombolysis and endovascular therapy.[3] The prompt reopening of obstructed vessels serves to salvage the ischemic penumbra. However, due to strict eligibility criteria, including imaging characteristics and a narrow therapeutic time window, only a minority of stroke patients qualify for intravenous thrombolysis, endovascular clot retrieval, or a combination of both therapies. Hence, there is a pressing demand for adjuvant neuroprotective therapy.[4] Diverging from exogenous or indirect neuroprotection strategies primarily focused on the cerebrovascular system, such as averting thrombus formation or disassembling existing clots, neuroprotection is defined as “neuronal preservation.” The objective of employing neurotrophic drugs for neuroprotection is to intervene in the pathological biochemical cascade within the ischemic penumbra, thereby preventing or delaying neuronal cell death.[5] Cerebrolysin, one of the neurotrophic drugs, consists of a mixture of low molecular weight porcine-derived peptides and free amino acids.[6] Currently, Cerebrolysin is primarily used to treat cerebral ischemia and neurodegenerative diseases.[7] However, despite numerous trials, the current guidelines do not strongly recommend or discourage its use.[8–10]
Health technology assessment (HTA) provides decision-makers with insights to facilitate the establishment of an equitable, efficient, and high-quality healthcare system.[11] The process entails a comprehensive evaluation of the technical characteristics, clinical safety, effectiveness, economic impact, equity, and ethical considerations associated with healthcare technology.[12] However, one drawback of HTA is its potential for being time-consuming. In contrast, the Rapid Health Technology Assessment (RHTA) entails swiftly evaluating a specific health technology’s efficacy, safety, and cost-effectiveness. Typically completed within 1 to 6 months, RHTA enables the timely provision of crucial information for informed policy decisions while encompassing all essential aspects expected from a comprehensive review.[13] This study was expected to evaluate the efficacy, safety, and cost-effectiveness of adjuvant treatment of AIS with Cerebrolysin by RHTA to provide evidence-based evidence for the rational clinical use of Cerebrolysin.
2. Methods 2.1. Inclusion and exclusion criteria 2.1.1. Types of research.We included published systematic reviews (SR) or meta-analyses, pharmacoeconomic studies, and HTA reports.
2.1.2. Research subjects.The study population was patients who met the diagnostic criteria for AIS.[14]
2.1.3. Interventions.The treatment group consisted of Cerebrolysin monotherapy or a combination with conventional treatment. The control group received either conventional treatment, placebo combined with conventional treatment, or other neurotrophic drugs along with conventional treatment. The treatment and control groups had no limitations on drug dosage or duration.
Conventional treatment was defined as pharmacological and non-pharmacological treatments excluding neuroprotective agents, including improvement of cerebral blood circulation (intravenous thrombolysis, endovascular therapy, antiplatelet treatment, antithrombotic treatment, fibrinolysis therapy, volume expansion, etc.) and symptomatic treatments (respiration and supplemental oxygen, cardiac monitoring, temperature control, blood pressure control, plasma glucose control, and lipid control, etc.).[9]
2.1.4. Outcome indicators.Efficacy indicators include overall clinical efficacy rate, cure rate, neurological deficit assessment, stroke-related motor outcome measure, daily living ability assessment, hemorheology-related indicators, etc. Safety indicators include the incidence of all-cause mortality, adverse reactions (AR), adverse events (AE), serious adverse reactions (SAR), serious adverse events (SAE), disability rate, etc. Economic indicators include the cost-effectiveness ratio and the incremental cost-effectiveness ratio.
2.1.5. Exclusion criteria.The exclusion criteria were as follows: study population: literature on clinical studies not targeting IS, such as neonatal hypoxic-ischemic encephalopathy and acute hemorrhagic stroke; study measures: the combination of drugs (Cerebrolysin combined with Shuxuetong injection, etc.) and combination of non-pharmacological treatments (hyperbaric oxygen, etc.); updated literature published by the same author in different years, taking the latest; and irrelevant literature, reviews, conference abstract, literature with lack of data or inability to obtain the complete text, and animal experiments, etc.
2.2. Search strategyWe searched databases including PubMed, Embase, the Cochrane Library, China National Knowledge Infrastructure, Wanfang, Weipu, and SinoMed. Meanwhile, we searched for HTA in the International Network of Agencies for Health Technology Assessment, International Society of Technology Assessment in Health Care, and Health Technology Assessment international (HTAi). We were conducted using “stroke, Cerebrolysin, Pharmacy Economic, Meta-Analysis, etc.” as subject terms, with a search time frame from the date of database inception to August 17, 2023. In addition, the references of the included studies were manually searched to ensure completeness. The search strategy is shown in Table S1, Supplemental Digital Content, https://links.lww.com/MD/L981, using PubMed as an example.
2.3. Literature screeningAfter deduplication using Endnote X9, two researchers (M.W. and K.Y.) independently screened and crosschecked literature by reading the title, abstract, and full text according to the inclusion and exclusion criteria. If there were any disagreement, they would negotiate with the third researcher.
2.4. Literature extractionIt was independently extracted by 2 researchers (M.W. and K.Y.) in accordance with a predesigned data extraction form. Table 1 presents the essential characteristics of systematic evaluations/meta-analysis that reflect effectiveness and safety, including the first author, publication year, type of study, number of people in the study, intervention vs. control comparisons, risk of bias assessment methods, etc. The primary characteristics of pharmacoeconomic studies reflecting economy are shown in Table 2, consisting of the first author, publication year, geographical region, research perspective, intervention vs. control comparisons, research methodology, etc.
Table 1 - Summary of included SRs/meta-analyses. Study Research type Retrieval date Study population Intervention measure Bias risk assessment method No. (cases) Total cases Efficacy outcome index Safety outcome index Comparison group Control group Zhang, D 2017[15] Meta-analysis 2016.7 Acute ischemic stroke Cerebrolysin monotherapy or combination with conventional treatment Placebo or placebo + conventional treatment Cochrane Risk of bias tool 7 1779 (5)(6) (8)(9)(10) Wang, Z 2017[16] Meta-analysis 1980.1–2016.5 Acute ischemic stroke Cerebrolysin in combination with conventional treatment Placebo + conventional treatment Cochrane Risk of bias tool 6 1649 (2)(5)(6) (8)(9)(10) Bornstein, N. M 2017[17] Meta-analysis 2016.12.31 Acute ischemic stroke Cerebrolysin in combination with conventional treatment Placebo + conventional treatment Jadad scale 9 1879 (2)(6) (8)(9)(10) Guekht, A 2017[18] Meta-analysis / Acute ischemic stroke Cerebrolysin Placebo Not reported 2 448 (2)(4) (8)(9)(10)Other neurotrophic drugs are Citicoline, Edaravone, etc.
The methodological quality of the included SR or meta-analyses was evaluated using the A Measure Tool to Assess Systematic Reviews 2 (AMSTAR 2) scale, consisting of 16 items, with items 2, 4, 7, 9, 11, 13, and 15 considered vital items.[31] The quality of the pharmacoeconomic studies was assessed using the Consolidated Health Economic Evaluation Reporting Standards (CHEERS 2022) checklist.[32]
2.6. Data consolidation and analysisWe conducted a literature review, analyzed the fundamental characteristics of the included studies, and summarized the results using a combination of descriptive analysis and tables.
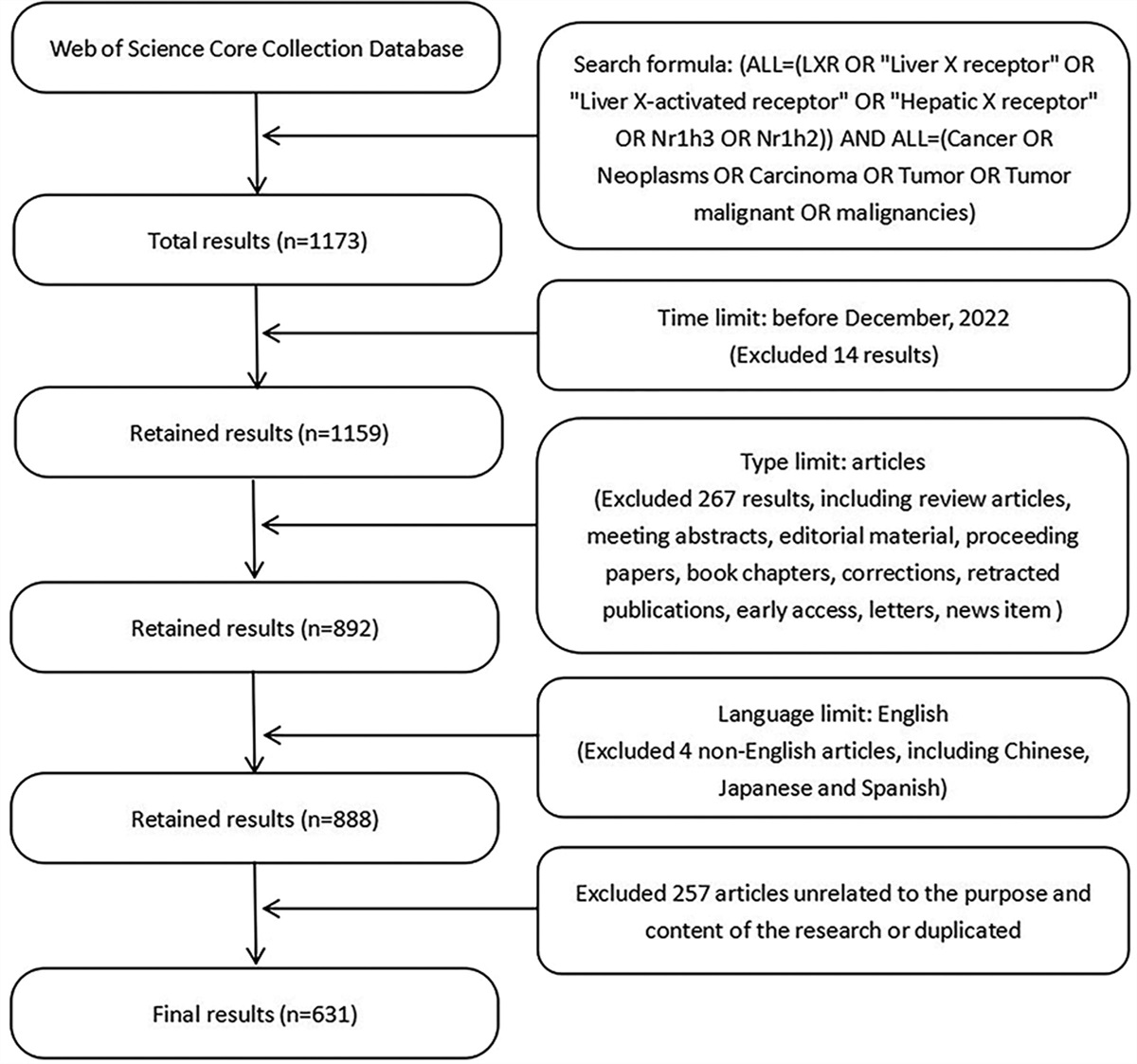
3. Result 3.1. Literature search resultsIn the initial retrieval, a total of 188 articles were identified. After layer-by-layer screening according to the inclusion and exclusion criteria, a final set of 14 articles was included, including 8 SR or meta-analysis[15–22] and 6 pharmacoeconomic studies.[25–30] No HTA report was retrieved. The literature screening process and results are provided in Figure 1.
 Figure 1.:
Figure 1.: Literature screening flow chart.
3.2. Main characteristics of the included literatureThe main features of the included studies are reported in Tables 1 and 2.
3.3. Quality evaluation of included studies 3.3.1. Quality evaluation of SR/meta-analysis.Seven SR/meta-analyses were included in the study, and the indicators of clinical effectiveness evaluation included: Overall clinical efficacy rate; Neurological deficit assessment: National Institutes of Health Stroke Scale(NIHSS) Score and Modified Edinburgh-Scandinavian Stroke Scale (MESSS) Score; Stroke-related motor outcome measures: The Action Research Arm Test (ARAT) Scale;[23] Daily living ability assessment: Barthel Index Scale(BI) score and modified Rankin Scale(mRS) score;[24] and Hemorheology related indicators: whole blood viscosity, plasma viscosity, and fibrinogen content. Safety indicators include disability rate, mortality rate, AE, SAE, AR, SAR etc. We utilized the AMSTAR2 scale to assess the quality of the included studies. The quality evaluation results of the SR/Meta-analysis are shown in Table 3
Table 3 - Quality evaluation of included SR/meta-analysis. Items Study Zhang, D 2017[15] Wang, Z 2017[16] Bornstein, NM 2017[17] Guekht, A 2017[18] Tang, R 2017[19] Yu, F 2018[20] Ziganshina, LE 2020[21] Strilciuc, S 2021[22] 1. Did the research questions and inclusion criteria for the review include the components of PICO? Y Y Y Y Y Y Y Y 2. Did the report of the review contain an explicit statement that the review methods were established prior to the conduct of the review and did the report justify any significant deviations from the protocol? N PY PY N N N Y Y 3. Did the review authors explain their selection of the study designs for inclusion in the review? N N N Y N N Y N 4. Did the review authors use a comprehensive literature search strategy? PY N Y N PY N Y Y 5. Did the review authors perform study selection in duplicate? Y Y Y N Y Y Y Y 6. Did the review authors perform data extraction in duplicate? N Y Y N N Y Y Y 7. Did the review authors provide a list of excluded studies and justify the exclusions? N N N N N N Y N 8. Did the review authors describe the included studies in adequate detail? Y Y Y PY N PY Y Y 9. Did the review authors use a satisfactory technique for assessing the risk of bias (RoB) in individual studies that were included in the review? Y Y Y N Y Y Y Y 10. Did the review authors report on the sources of funding for the studies included in the review? N N N N N N Y N 11. If meta-analysis was performed did the review authors use appropriate methods for statistical combination of results? Y Y Y Y N N Y Y 12. If meta-analysis was performed, did the review authors assess the potential impact of RoB in individual studies on the results of the meta-analysis or other evidence synthesis? N N Y Y N N Y Y 13. Did the review authors account for RoB in individual studies when interpreting/discussing the results of the review? Y N N N Y Y Y Y 14. Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the results of the review? Y Y Y Y N N Y Y 15. If they performed quantitative synthesis did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the results of the review? Y Y Y N N N Y N 16. Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review? Y Y N Y N N Y Y The number of key items not compliant 2 3 2 6 4 5 0 2 The number of non-key items not compliant 4 3 3 3 7 5 0 2 Grades Critically low Critically low Critically low Critically low Critically low Critically low High Critically lowYes (Y): The report content adheres to the standard of a specific item on the AMSTAR2 scale; Partial Yes (PY): The report content is not comprehensive and partially adheres to the standard of a specific item on the AMSTAR2 scale; No (N): The report content does not comply with the standard of a specific item on the AMSTAR2 scale.
Following the evaluation criteria outlined in the AMSTAR 2 guidelines,[31] the results indicate that, with the exception of one Cochrane systematic review assessed as “high” quality, the quality of the remaining included literature is categorized as “critically low.” The primary factors contributing to the low methodological quality of the included studies are as follows: the report of the review did not state an explicit statement that the research methods for the systematic review had been established prior to its implementation[15,18–20]; lack of comprehensiveness in the literature retrieval strategies[16,18,20]; except for a few studies,[21] the review authors did not provide a list of excluded studies and justify the exclusions; there were incomplete items to assess the risk of bias[18]; the review authors did not describe the reason of combining the data in a meta-analysis[19]; the effect of the risk of bias on the results was not discussed[16–18]; the publication bias was not reported[18,22] or the severity degree of the impact of publication bias was not discussed.[19]
3.3.2. Quality evaluation of economic research.Including 6 pharmacoeconomic evaluations, the efficacy indicators comprised changes between pre-and post-treatment NIHSS scores, BI index, the total effective rate assessed according to the Degree of clinic neurological function deficit scale (NDS) in Stroke Patients (1995), and so on. Economic evaluation indicators encompassed the cost-effectiveness ratio (C/E) and the incremental cost-effectiveness ratio (△C/△E), among others. The quality evaluation results of economic research are shown in Table 4.
Table 4 - Quality evaluation of included pharmacoeconomic studies. Items Study Lin WS 2004[25] Zhang GX 2010[26] Li G 2013[27] Men P 2016[28] He X 2017[29] Strilciuc S 2023[30] 1. Title PC PC C C C C 2. Abstract C C C C C C 3. Background and objectives PC PC PC C C C 4. Health economic analysis plan NR NR NR NR NR NR 5. Study population
Comments (0)