
Remember me



Isolated patellofemoral osteoarthritis is thought to occur in 11 to 24% of patients aged 55 years or older with knee pain.1,2 In these cases, isolated patellofemoral arthroplasty (PFA) may be considered and allows for ligamentous as well as tibiofemoral joint preservation.3 However, this is less studied than other related procedures.
First introduced in the 1970's,4 PFA has historically been viewed with controversy because of inconsistent success and high failure rates reported among first-generation implants.5–8 Despite this, newer, second-generation implants are viewed more favorably.9 PFA with modern implants may enable a shorter time to recovery with similar outcomes,10 lower revision rates,11 improved knee-related quality of life,12 lower cost,13 and better range of motion at 2 years12 when compared with total knee arthroplasty (TKA). As such, PFA is becoming an increasingly popular option for the treatment of isolated patellofemoral arthritis.6,14
While clinical outcomes of PFA have been studied, other outcome metrics have received less attention. To that end, postoperative emergency department (ED) visits after surgery are a metric of quality of care,15–17 higher healthcare costs,18 and lesser patient satisfaction,19 which are gaining increased attention in the orthopaedic literature. Thus, as the Centers for Medicare & Medicaid Services expand systems aimed at providing value-based care, strategies to provide high-quality, highly cost-effective care in the postoperative setting are particularly important.20 Despite this, while the incidence, timing, and reasons for postoperative ED visits have been studied in a number of common orthopaedic procedures,15–17 characterization of these in the postoperative period after PFA is still lacking.
To address the abovementioned gap in the literature, this study was conducted to characterize the incidence, timing, and reasons for ED visits after PFA. A large, national, administrative database was used to leverage the power afforded by a large patient sample. In addition to helping inform preoperative counseling, these data may also help with the evolution of targeted postoperative care pathways.
Methods Database and CohortThe 2010 to 2021 PearlDiver M151Ortho data set was used. This is a large, Health Insurance Portability and Accountability Act–compliant, national health administrative data set containing claims information on over 151 million orthopaedic patients in the United States. PearlDiver data are collected across all sites of care in the United States and across payer types and provider specialties. As PearlDiver query outputs are aggregate and deidentified, our institutional review board determined studies using this database exemption from review.
PFA patients were identified by the Current Procedural Terminology (CPT) code 27438. Any patient with a diagnosis of trauma, neoplasm, or infection on the day of surgery or without at least 90 days of follow-up in the data set after PFA was excluded from this study.
After patient identification, patient characteristics were determined and tabulated, including age, sex, Elixhauser Comorbidity Index (ECI, a patient comorbidity index constructed using International Classification of Diseases [ICD] diagnosis codes), region of the country where surgery was performed (Midwest, Northeast, South, or West), patient insurance plan (commercial, Medicaid, or Medicare), and postoperative length of stay (1+ night(s), same-day discharge).
Emergency Department Utilization/ReadmissionsEmergency department utilization in the 90 days after PFA was characterized by identification of ED visit–specific codes CPT-99281, CPT-99282, CPT-99283, CPT-99284, and CPT-99285. Both the total number of ED visits and weekly ED visits were determined. To characterize a baseline rate of ED utilization for the study cohort, the average incidence of ED utilization from weeks 52 to 56 after PFA was determined. Only patients with a minimum of 56 weeks of follow-up after PFA were included in this analysis.
The primary diagnosis for ED visit was characterized based on primary associated ICD codes for the ED visits. These were manually grouped and characterized as postoperative pain, surgical site infection, swelling/effusion, wound complications/care, cardiovascular, gastrointestinal, central nervous system/psychiatric, or other. These categories were grouped as being related to the surgical site (pain, infection, swelling, wound complications) or unrelated to the surgical site (cardiovascular, gastrointestinal, central nervous system, other).
Data AnalysisUnivariate analysis was used to analyze patient characteristics of PFA patients who did and did not visit the ED after surgery. Pearson chi square test was used to evaluate differences in sex, region, insurance plan, and postoperative length of stay between the two groups. Welch t-test was performed to determine differences in average age and ECI in the two groups.
Multivariate logistic regression was conducted to identify independent predictive factors for postoperative ED utilization. Odds ratios (OR) and 95% confidence intervals (CIs) were determined for each factor analyzed and compared with their respective referent categories.
PearlDiver's built-in statistics package was used to conduct all statistical analyses in this study—with statistical significance reached at P < 0.05. Prim9 (GraphPad Softwares) and Microsoft Excel (Microsoft Corporation, Redmond, WA) were used to create all figures.
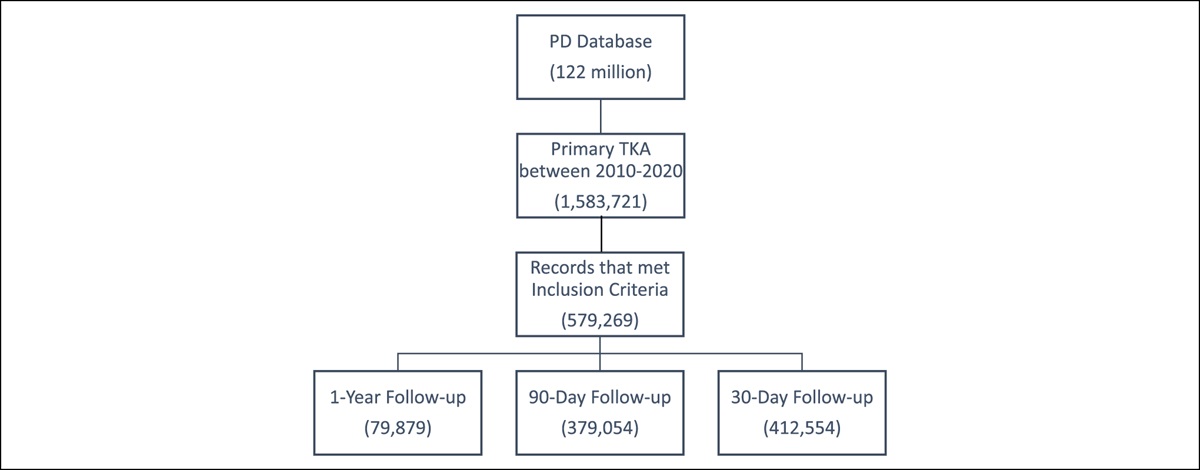
Results Study Cohort and Incidence of Emergency Department UtilizationA total of 7765 PFA patients were identified based on inclusion/exclusion criteria, of which 992 (11.2%) visited the ED within 90 days of surgery. The overall occurrence and weekly incidence of ED utilization after PFA are shown in Figure 1. Of the 922 patients who visited the ED, one visit was recorded for 709 patients, two visits for 149 patients, three visits for 39 patients, and 4+ visits for 26 patients.
 Figure 1:
Figure 1: Bar graph depicts the weekly incidence of emergency department (ED) visits after patellofemoral arthroplasty. Pie chart shows the breakdown of patients who visited versus did not visit the ED after surgery. The baseline for weekly ED visit incidence was calculated by averaging weekly visits between 52 and 56 weeks after total ankle arthroplasty.
Of all ED visits in the 90 days after PFA, nearly half (46.7%) occurred in the first 3 weeks after surgery. Emergency department visits were noted during the first postoperative week for 225 patients (2.90% of the study cohort) visited the ED, during the second postoperative week for 121 (1.56%), and during the third postoperative week for 85 (1.09%). For reference, the baseline weekly ED utilization for the study cohort approximately 1 year after surgery (ie, weeks 52 to 56) was (average ± standard deviation) 0.18% ± 0.07%.
In contrast to the 11.2% of patients who visited the ED in the 90 days after PFA, readmissions were noted during the same interval for 280 patients (3.61% of the study population and 30.4% of those who presented to the ED).
Predictive Factors for Postoperative Emergency Department UtilizationDemographic factors of the PFA study cohort are summarized in Table 1. In this population of 7765 PFA patients, the average ± SD age was 56.0 ± 12.5 years, with female patients constituting a large majority (72.2% female versus 27.8% male). The comorbidity burden of the overall study cohort was low to moderate, with an average ± SD ECI of 3.6 ± 3.1. PFA was most performed in the Southern United States (37.1%) and least commonly performed in the West (15.0%). Most PFA patients were commercially insured (72.8%), with much smaller proportions having Medicare (18.8%) or Medicaid (4.6%) coverage. PFA was more commonly performed as an inpatient procedure, with 53.7% of patients having a postoperative length of stay greater than or equal to one night compared with 46.3% of patients who were discharged on the same day as surgery.
Table 1 - Univariate Analysis of Characteristics of Patients With Patellofemoral Arthroplasty Total No ED Visit ED Visit P N 7765 6843 922 Age (mean ± SD) 56.0 ± 12.5 56.5 ± 12.3 52.6 ± 13.0 <0.0001 <30 86 (1.1%) 68 (1%) 17 (1.8%) 30-39 667 (8.6%) 515 (7.5%) 149 (16.2%) 40-49 1768 (22.8%) 1527 (22.3%) 240 (26%) 50-59 2160 (27.8%) 1928 (28.2%) 231 (25.1%) 60-69 1703 (21.9%) 1553 (22.7%) 154 (16.7%) >69 1381 (17.8%) 1252 (18.3%) 131 (14.2%) Sex 0.3098 Female 5605 (72.2%) 4926 (72%) 679 (73.6%) Male 2160 (27.8%) 1917 (28%) 243 (26.4%) ECI (mean ± SD) 3.6 ± 3.1 3.4 ± 2.9 5.5 ± 3.6 <0.0001 0-1 2214 (28.5%) 2097 (30.6%) 100 (10.8%) 2-3 2226 (28.7%) 1994 (29.1%) 208 (22.6%) 4-5 1614 (20.8%) 1392 (20.3%) 234 (25.4%) >5 1711 (22.0%) 1360 (19.9%) 360 (39.0%) Region 0.0009 Midwest 2299 (29.6%) 1989 (29.1%) 310 (33.6%) Northeast 1377 (17.7%) 1225 (17.9%) 151 (16.4%) South 2878 (37.1%) 2525 (36.9%) 354 (38.4%) West 1168 (15.0%) 1063 (15.5%) 105 (11.4%) Insurance <0.0001 Commercial 5655 (72.8%) 4999 (73.1%) 660 (71.6%) Medicaid 361 (4.6%) 273 (4%) 106 (11.5%) Medicare 1458 (18.8%) 1325 (19.4%) 131 (14.2%) Postoperative length of stay 0.0726 1+ Night(s) 4169 (53.7%) 3700 (54.1%) 469 (50.9%) Same-day discharge 3596 (46.3%) 3143 (45.9%) 453 (49.1%)Bold indicates statistical significance (P < 0.05).
The numbers of those without and with 90-day postoperative ED visits and univariate comparison are also presented in Table 1. All demographic factors analyzed were significantly associated with ED utilization in the 90 days after PFA (P < 0.0001 for age, ECI, and insurance; P = 0.0009 for region), except for patient sex (P = 0.3098) and postoperative length of stay (P = 0.0726).
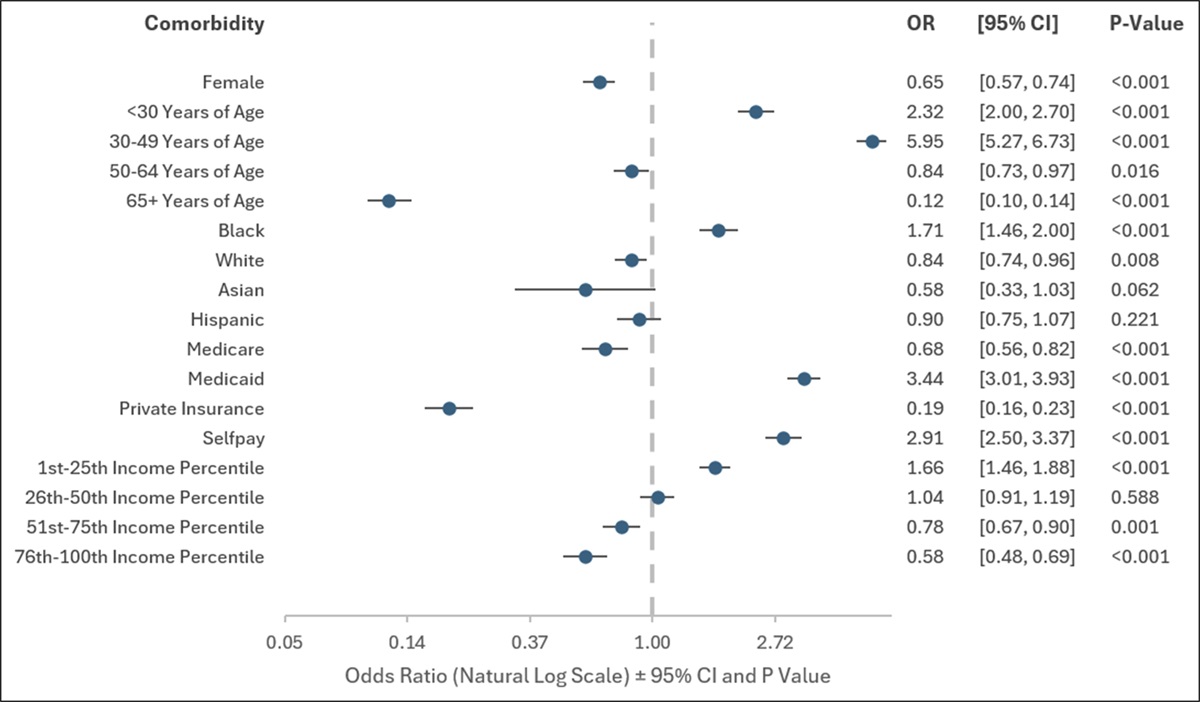
The results of multivariate logistic regression analysis for independent predictors of ED utilization after PFA are provided in Table 2 and visually represented in Figure 2. Several factors were independently associated with postoperative ED utilization, including younger age (per decade decrease, odds ratio [OR] 1.40; 95% CI = 1.31 to 1.49; P < 0.0001), higher ECI (OR 1.44; 95% CI = 1.38 to 1.50; P < 0.0001), having surgery performed in the South or Midwest (compared with Northeast, OR 1.27 and 1.31; 95% CI = 1.03 to 1.57 and 1.06 to 1.63; P = 0.0239 and P = 0.0145, respectively), or having Medicaid insurance (compared with Medicare, OR 1.74; 95% CI = 1.25 to 2.41; P < 0.0001).
Table 2 - Multivariate Analysis of Predictive Factors for Emergency Department (ED) Utilization N = 7765 OR (95% CI) P Age (per decade decrease) 1.40 (1.49, 1.31) <0.0001 Sex Male (referent) Female 1.08 (0.92, 1.27) 0.3455 ECI (per 2-point increase) 1.44 (1.38, 1.50) <0.0001 Region Northeast (referent) West 1.02 (0.78, 1.34) 0.8863 South 1.27 (1.03, 1.57) 0.0237 Midwest 1.31 (1.06, 1.63) 0.0141 Insurance Medicare (referent) Commercial 1.03 (0.83, 1.28) 0.8191 Medicaid 1.74 (1.25, 2.41) 0.0011 Postoperative length of stay 1+ Night(s) (referent) Same-day discharge 1.00 (0.87, 1.15) 0.9952Bold indicates statistical significance (P < 0.05).
 Figure 2:
Figure 2: Forest plot depicting results of multivariate analysis for independent predictive factors for emergency department (ED) utilization within 90 days of patellofemoral arthroplasty. Error bars represent 95% confidence intervals (CIs). Black bars indicate statistical significance (P < 0.05).
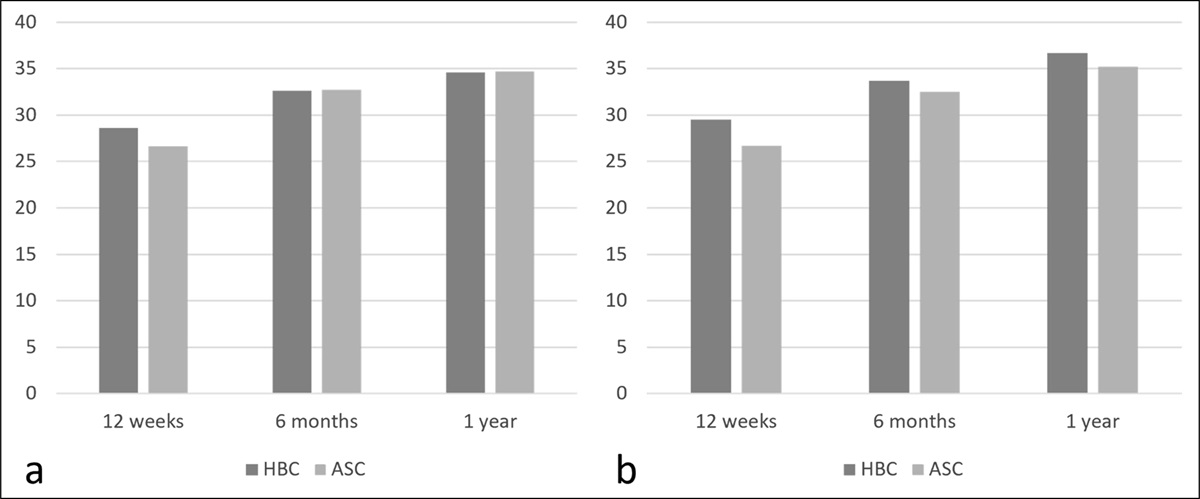
Reasons for Postoperative Emergency Department UtilizationThe primary reasons for ED visits in the 90 days after PFA are shown in Figure 3. Reasons for ED utilization that were characterized as directly related to the surgical site (66% of ED visits) included postoperative pain (50.6%), surgical site infection (9.1%), swelling/effusion (4.0%), and wound complications/care (1.9%). Emergency department visits for reasons characterized as unrelated to the surgical site (34% of ED visits) included cardiovascular (11.6%), gastrointestinal (10.8%), central nervous system/psychiatric (10.2%), and “other” (1.7%).
 Figure 3:
Figure 3: Bar graph and pie chart showing the most frequent primary diagnosis among patellofemoral arthroplasty patients who visited the emergency department (ED) within 90 days of surgery divided by relation to the surgical site.
DiscussionCurrently, relatively little literature exists regarding various PFA outcomes. This study aimed to address some of this gap by examining the 90-day post-PFA ED visits. To do this, a large, administrative database was leveraged to study 7765 PFA patients, which we believe to be the largest PFA study cohort to date.13,21–25
Of the 7765 patients, 992 (11.2%) visited the ED within 90 days of their surgery. This is comparable with previously reported rates of 90-day ED utilization after TKA—at approximately 10.8%.26 A recent PearlDiver study reported higher postoperative ED utilization after TKA (6.1%), compared with PFA (3.9%)27; however, this study was limited to the period 2010 to 2015 and only included TKA procedures performed for isolated patellofemoral arthritis. Furthermore, this study matched TKA and PFA patients by age, sex, and comorbidity burden—all these factors may have led to differential rates of postoperative ED utilization when compared with our study. For timing, nearly half of these patients (46.7%) visited the ED within the first 3 weeks, 21.6% had more than one ED visit, and a high percentage of patients had more than one ED visit. Notably, 280 patients (3.61% of the study cohort) were readmitted during the same interval, a small fraction of the patients who presented to the ED postoperatively. Together, these data highlight that post-PFA ED visits are an outcome measure in need of attention.
The multivariable analysis identified factors independently predictive of such ED visits. Overall, younger age, increased ECI, South and Midwest regions, and Medicaid were markedly predictive of postoperative ED visits.
Younger patients were found to have 1.40 higher odds per decade decrease of visiting the ED after a PFA. Although this may seem counterintuitive, prior studies examining total knee and hip arthroplasty, ankle fracture surgery, and anterior cruciate ligament reconstruction found similar findings.17,28,29 This may be contributed to by the effect of pain on younger versus older populations,30 and it should be noted that comorbidities were separately accounted for by the multivariate analysis. In fact, ECI was associated with 1.44 higher odds per two-point increase of presenting to the ED. This trend is more intuitive and is likely due to patients with higher comorbidities being at increased risk of complications.31,32
In examining regional differences in the United States (with the Northeast as the referent), higher odds of post-PFA ED visits were noted for those from the South (1.27) and Midwest (1.31). This geographic trend may be contributed to by differential thresholds for ED utilization trends in different parts of the country and is consistent with regional variations in ED utilization identified in prior studies.29,33 Nonetheless, the largest predictive factor was patients with Medicaid insurance (with Medicare as the referent) who had 1.74 higher odds of having an ED visit. This finding was of age and ECI and again consistent with trends from prior literature.34,35 This could be related to differential healthcare access and copay exemption in the ED.
In examining the reasons for ED visits after a PFA, the most common reason was related to the surgical site (66%). Within this, the most common reason was due to postoperative pain, which is consistent with prior studies.14,15 This suggests that one of the primary focuses to reduce ED utilization after PFA would be to focus on a pain management regimen and/or education on pain management. Following postoperative pain, the next most common reason for an ED visit related to the surgical site was surgical site infection. This is an important metric to consider because surgical site infections have been found in prior orthopaedic studies to be associated with increased morbidity and healthcare utilization.36–39
There are limitations to this study. One limitation is that this study used an administrative database and thus is reliant on the accuracy of the coded data. The next limitation is that there are multiple reasons why patients visit the ED, but our data only examined the primary diagnosis associated with a patient's ED visit.
In conclusion, this study used a large, administrative database to examine a large cohort of 7765 PFA patients to better understand trends and reasons for postoperative ED visits after surgery. Of these patients, 11.2% visited the ED within 90 days of their surgery, almost half (46.7%) visited within the first 3 weeks, and postoperative pain was the most common reason. By identifying the timing of ED visits as well as the predisposing factors and reasons for ED visits in this patient population, care pathways may be able to be adjusted to reduce ED visits and minimize healthcare burden associated with patellofemoral arthroplasties.
References 1. Davies AP, Vince AS, Shepstone L, Donell ST, Glasgow MM: The radiologic prevalence of patellofemoral osteoarthritis. Clin Orthop Relat Res 2002:206-212. 2. McAlindon TE, Snow S, Cooper C, Dieppe PA: Radiographic patterns of osteoarthritis of the knee joint in the community: The importance of the patellofemoral joint. Ann Rheum Dis 1992;51:844-849. 3. Gupta RR, Zywiel MG, Leadbetter WB, Bonutti P, Mont MA: Scientific evidence for the use of modern patellofemoral arthroplasty. Expert Rev Med Devices 2010;7:51-66. 4. Blazina ME, Fox JM, Del Pizzo W, Broukhim B, Ivey FM: Patellofemoral replacement. Clin Orthop Relat Res 1979:98-102. 5. Hassaballa MA, Porteous AJ, Newman JH: Observed kneeling ability after total, unicompartmental and patellofemoral knee arthroplasty: Perception versus reality. Knee Surg Sports Traumatol Arthrosc 2004;12:136-139. 6. Leadbetter WB, Ragland PS, Mont MA: The appropriate use of patellofemoral arthroplasty: An analysis of reported indications, contraindications, and failures. Clin Orthop Relat Research® 2005;436:91-99. 7. Hendrix MRG, Ackroyd CE, Lonner JH: Revision patellofemoral arthroplasty: Three- to seven-year follow-up. J Arthroplasty 2008;23:977-983. 8. van Jonbergen H-PW, Werkman DM, Barnaart AFW: Dissociation of mobile-bearing patellar component in low contact stress patellofemoral arthroplasty, its mechanism and management: Two case reports. Cases J 2009;2:7502. 9. Dy CJ, Franco N, Ma Y, Mazumdar M, McCarthy MM, Gonzalez Della Valle A: Complications after patello-femoral versus total knee replacement in the treatment of isolated patello-femoral osteoarthritis. A meta-analysis. Knee Surg Sports Traumatol Arthrosc 2012;20:2174-2190. 10. Dahm DL, Al-Rayashi W, Dajani K, Shah JP, Levy BA, Stuart MJ: Patellofemoral arthroplasty versus total knee arthroplasty in patients with isolated patellofemoral osteoarthritis. Am J Orthop 2010;39:487-491. 11. Peng G, Liu M, Guan Z, et al.: Patellofemoral arthroplasty versus total knee arthroplasty for isolated patellofemoral osteoarthritis: A systematic review and meta-analysis. J Orthop Surg Res 2021;16:264. 12. Odgaard A, Madsen F, Kristensen PW, Kappel A, Fabrin J: The mark coventry award: Patellofemoral arthroplasty results in better range of movement and early patient-reported outcomes than TKA. Clin Orthop Relat Res 2018;476:87-100. 13. Fredborg C, Odgaard A, Sørensen J: Patellofemoral arthroplasty is cheaper and more effective in the short term than total knee arthroplasty for isolated patellofemoral osteoarthritis: Cost-effectiveness analysis based on a randomized trial. Bone Joint J 2020;102-b:449-457. 14. Lonner JH: Patellofemoral arthroplasty. JAAOS - J Am Acad Orthop Surg 2007;15:495-506. 15. Kammien AJ, Galivanche AR, Gouzoulis MJ, Moore HG, Mercier MR, Grauer JN: Emergency department visits within 90 days of single-level anterior cervical discectomy and fusion. N Am Spine Soc J 2022;10:100122. 16. Kammien AJ, Zhu JR, Gouzoulis MJ, et al.: Emergency department visits within 90 Days of anterior cruciate ligament reconstruction. Orthop J Sports Med 2022;10:23259671221083586. 17. Finnegan MA, Shaffer R, Remington A, Kwong J, Curtin C, Hernandez-Boussard T: Emergency department visits following elective total hip and knee replacement surgery: Identifying gaps in continuity of care. J Bone Joint Surg Am 2017;99:1005-1012. 18. Galarraga JE, Pines JM: Costs of ED episodes of care in the United States. Am J Emerg Med 2016;34:357-365. 19. Thompson DA, Yarnold PR, Williams DR, Adams SL: Effects of actual waiting time, perceived waiting time, information delivery, and expressive quality on patient satisfaction in the emergency department. Ann Emerg Med 1996;28:657-665. 20. Bundled Payments for Care Improvement (BPCI) Initiative: General Information. Available at: https://innovation.cms.gov/innovation-models/bundled-payments 21. Clement ND, Howard TA, Immelman RJ, et al.: Patellofemoral arthroplasty versus total knee arthroplasty for patients with patellofemoral osteoarthritis: Equal function and satisfaction but higher revision rate for partial arthroplasty at a minimum eight years' follow-up. Bone Joint J 2019;101-b:41-46. 22. Kooijman HJ, Driessen AP, van Horn JR: Long-term results of patellofemoral arthroplasty. A report of 56 arthroplasties with 17 years of follow-up. J Bone Joint Surg Br 2003;85:836-840. 23. Arciero RA, Toomey HE: Patellofemoral arthroplasty. A three- to nine-year follow-up study. Clin Orthop Relat Res 1988:60-71. 24. Argenson JN, Guillaume JM, Aubaniac JM: Is there a place for patellofemoral arthroplasty?. Clin Orthop Relat Res 1995:162-167. 25. Lewis PL, Tudor F, Lorimer M, et al.: Short-term revision risk of patellofemoral arthroplasty is high: An analysis from eight large arthroplasty registries. Clin Orthop Relat Res 2020;478:1222-1231. 26. Maldonado-Rodriguez N, Ekhtiari S, Khan MM, et al.: Emergency department presentation after total hip and knee arthroplasty: A systematic review. J Arthroplasty 2020;35:3038-3045. 27. Serino J 3rd, Weintraub MT, Burnett RA 3rd, Angotti ML, Courtney PM, Della Valle CJ: Complications and costs of patellofemoral arthroplasty versus total knee arthroplasty. Knee 2023;41:58-65. 28. Prather J, Alexander B, Halstrom J, et al.: Factors affecting emergency department visits, readmissions, and reoperations within 30 days of ankle fracture surgery- an institutional retrospective study. Injury 2020;51:2698-2702. 29. Kammien A: Emergency department visits within ninety days of anterior cruciate ligament reconstruction. 2022. 30. Gibson SJ, Helme RD: Age-related differences in pain perception and report. Clin Geriatr Med 2001;17:433-456. 31. Ranson WA, Neifert SN, Cheung ZB, Mikhail CM, Caridi JM, Cho SK: Predicting in-hospital complications after anterior cervical discectomy and fusion: A comparison of the elixhauser and charlson comorbidity indices. World Neurosurg 2020;134:e487-e496. 32. Maron SZ, Neifert SN, Ranson WA, et al.: Elixhauser comorbidity measure is superior to charlson comorbidity index in-predicting hospital complications following elective posterior cervical decompression and fusion. World Neurosurg 2020;138:e26-e34. 33. Macht R, George J, Ameli O, Hess D, Cabral H, Kazis L: Factors associated with bariatric postoperative emergency department visits. Surg Obes Relat Dis 2016;12:1826-1831. 34. Raji Y, Vakharia AM, Chen M, et al.: Emergency department utilization is low after outpatient elective rotator cuff repair. J Am Acad Orthop Surg 2022;30:e547-e560. 35. Sivasundaram L, Trivedi NN, Kim CY, et al.: Emergency department utilization after elective hip arthroscopy. Arthroscopy 2020;36:1575-1583. 36. Senthi S, Munro JT, Pitto RP: Infection in total hip replacement: meta-analysis. Int Orthop 2011;35:253-260. 37. Glazebrook MA, Arsenault K, Dunbar M: Evidence-based classification of complications in total ankle arthroplasty. Foot Ankle Int 2009;30:945-949. 38. Hernández-Vaquero D, Fernández-Fairen M, Torres A, et al.: Treatment of periprosthetic infections: An economic analysis. Scientific World J 2013;2013:821650. 39. Kurtz SM, Lau E, Schmier J, Ong KL, Zhao K, Parvizi J: Infection burden for hip and knee arthroplasty in the United States. J Arthroplasty 2008;23:984-991.
Comments (0)