
Remember me



Fractures of the calcaneus are the most common fractures of the tarsal bones and comprise approximately 2% of all fractures. Seventy percent of these fractures are displaced and intra-articular, most commonly occurring from a notable axial load such as a fall from height or motor vehicle accident.1 These displaced and intra-articular calcaneal fractures may lead to notable morbidity in patients including the development of posttraumatic subtalar arthritis.1,2 Management of calcaneal fractures is difficult because of their complexity, associated soft-tissue injuries, and lack of consistent imaging parameters to help guide treatment and predict outcomes.
Böhler's angle (BA) is the most used radiographic parameter for determining calcaneal derangement after injury.3 This radiographic line is drawn from the highest point of the anterior process of the calcaneus to the highest point of the posterior articular facet. A second line is then drawn from the highest point of the posterior articular facet to the highest point of the calcaneal tuberosity. Studies have shown a correlation between BA at time of injury and overall postoperative functional outcome.4–9
The benchmark in assessment of calcaneal fractures is the CT scan. The opportunity to view calcaneal fractures in 3D space allows for both a clearer understanding of the injury as well as formation of a surgical versus nonsurgical plan.10,11 Sanders classification of calcaneal fractures is one way surgeons can categorize calcaneal fractures on CT scan.2 This classification system categorizes calcaneal fractures by the number of articular fragments seen on coronal and axial CT of the widest undersurface of the posterior facet of the calcaneus. Type I fractures are nondisplaced, type II fractures are two-part or split fractures, type III are three-part or split depression fractures, and type IV are four-part or highly comminuted articular fractures. Through the utilization of fracture classification systems, physicians can predict treatment outcomes. For example, Swords et al12 demonstrated that the degree of anterior process comminution was an important prognostic determinant with increasing comminution associated with worsened functional outcome.
The aim of our study was to present a new technique of analyzing calcaneal fractures using the equatorial talar line (ETL) as a gross radiographic parameter to determine severity of facet depression and lateral wall incompetence. This radiographic parameter has the potential to be incorporated into early clinical assessments for patients with calcaneal fractures. The purpose of this study was to assess the reliability of the ETL as a sensitive radiographic parameter to predict Sanders type III and IV fractures as well as the presence of lateral wall blowout.
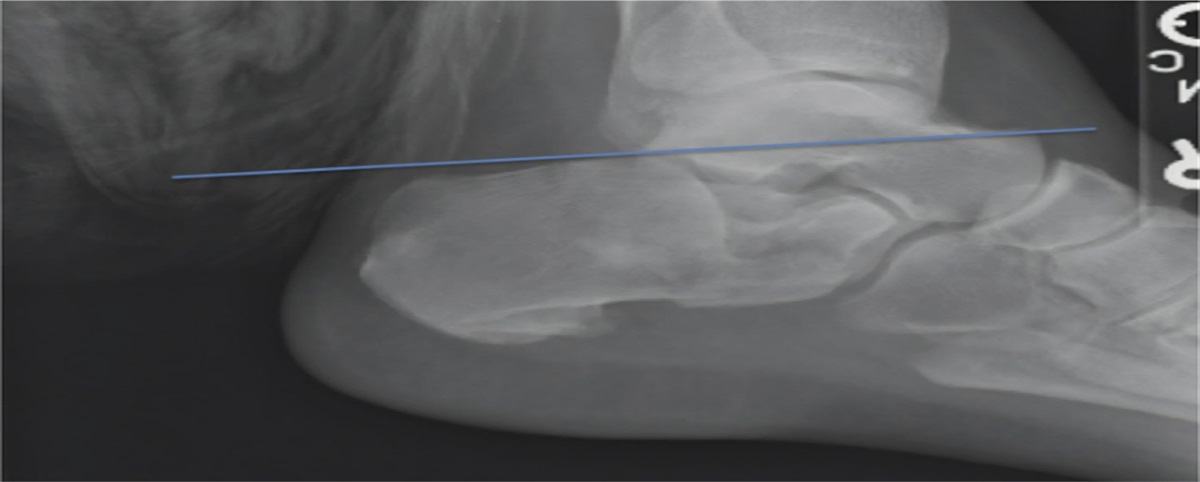
MethodsThe ETL (Figure 1) is defined as a line drawn from the most superior portion of the anterior process of the talar head through the most dorsal portion of the talar head and across the calcaneal tuberosity. This was the primary radiographic parameter used in the study.
 Figure 1:
Figure 1: Lateral radiograph of the ankle demonstrating the placement of the equatorial talar line.
Twenty-two depression-type calcaneus fractures from a single-institution level 1 trauma center were randomly selected, blinded, and further randomized for analysis. Lateral radiographs and coronal CT images of the calcaneus were selected. Two blinded trauma fellowship-trained surgeons, a senior resident, and a junior resident placed the ETL on each lateral radiograph and recorded the line as either “above” or “below” the posterior calcaneal tuberosity. If the line fell “above” the calcaneal tuberosity (Figure 2), a Sanders type I or II was predicted, whereas if the line fell “below” the calcaneal tuberosity (Figure 3), a higher grade, Sanders type III or IV was predicted. Furthermore, if the line fell “below” the tuberosity, lateral wall blowout was also expected. Lateral wall blowout is defined as the lateral calcaneal fragment displacing laterally beyond the fibula. The same blinded observers also classified each corresponding CT scan for Sanders classification and lateral wall blowout.
 Figure 2:
Figure 2: Lateral radiograph of the ankle demonstrating the equatorial talar line “above” the calcaneal tuberosity, predictive of Sanders type I or II fracture.
 Figure 3:
Figure 3: Lateral radiograph of the ankle demonstrating the equatorial talar line “below” the calcaneal tuberosity, predictive of Sanders type III or IV fracture.
Seven days later, all 22 fractures were then randomized again, and in a separate session, the same observers repeated the task, totaling 44 measurements for each radiograph and CT scan, respectively. Statistical analysis was conducted using SPSS 20.0. Reliability was calculated with the intraclass correlation coefficient (ICC), and a receiver operating curve (ROC) model was used to calculate predictive sensitivity.
ResultsIn determining the “above” or “below” location of the ETL, the calculated ICC was 1.0 for each session, as well as between both sessions. An ICC of 1.0 demonstrates a perfect correlation between groups. As a predictor of Sanders fracture classification type, the calculated ICC was 0.93 for session 1 and 0.89 for session 2 for an overall ICC of 0.91 between sessions 1 and 2 (Table 1). Three reviewers (75%) had no intraclass variability between sessions (Table 2).
Table 1 - Intraclass Correlation Coefficient Data Variable Location of ETL Predictor for Sanders Fracture Classification Session 1 1 0.93 Session 2 1 0.89 Overall ICC 1 0.91ETL = equatorial talar line, ICC = intraclass correlation coefficient
As a predictor of Sanders fracture classification type, ROC analysis yielded an overall sensitivity of 0.82. As a predictor of lateral wall blowout, ROC analysis yielded an overall sensitivity of 0.81.
DiscussionThe goal of calcaneal fracture management is achieving anatomic reduction, optimizing ambulation and overall foot functionality, and minimizing long-term complications. Our radiographic tool, the ETL, has the potential to help contribute toward these goals in management. Our analysis found that using the ETL was 82% sensitive for predicting Sanders classifications and 81% sensitive for predicting lateral wall blowout based on CT review. Furthermore, we calculated an ICC of 0.91 between the first and second session, which highlights the tool's reliability. Both attending and resident physicians can use this easily reproducible tool to reliably predict Sanders type III and IV calcaneal fractures. With high sensitivity and reproducibility, surgeons can use the ETL to help facilitate a quick assessment and plan in patients with calcaneal fractures.
To our knowledge, there has not been a similar parameter reported, and this study allows for a quick radiographic assessment using one line drawn on the lateral ankle radiograph that can guide clinical treatment. This radiographic parameter can help shed light on preoperative assessments before a CT has been obtained. The utility of this radiographic parameter can be called into question if the standard care of a calcaneal fracture is a CT scan. Although a CT scan may be necessary, our radiographic parameter allows for an earlier assessment to guide clinical treatment. This may be useful for patient triage as well as in medically underserved communities that may not have adequate access to advanced imaging. We hope to provide this radiographic parameter as an additional tool, rather than a substitute for a CT scan.
General limitations of this study include the risk of measurement error due to interobserver variability, improper alignment of the ankle during radiographs, and loss of bony landmarks due to trauma. Bujang et al13 used Power Analysis and Sample Size software to determine the necessity of seven subjects, providing two ratings, to reach a power of 80%. Although we only have four reviewers, this study is the initial step in providing a new radiographic parameter to guide calcaneal fracture treatment. Piovesana et al14 highlighted the potential for low reproducibility using Sanders classification for calcaneal fractures. We must emphasize the possibility of incorrect alignment of the foot in standard radiographs, leading to errors in measurement. Figure 3 presents some of the complexities of using the ETL on lateral ankle radiographs, as the talar domes are not perfectly superimposed. Touissaint et al5 found that oblique radiographs are often the norm in the setting of trauma because of difficulties in proper positioning of the injured extremity as well as limitations from splint materials. The authors also highlighted notable inaccuracies in the measurement of BA using these oblique lateral radiographs. To mitigate this concern, consistent limb positioning is crucial. Finally, the clinical utility of additional radiographic parameters can be called into question. Schepers et al15 explained that although the Sanders classification did not show a direct correlation with treatment, it did show positive correlation with outcome through the utilization of the Bernstein classification system. The Bernstein16 classification allows for the grading of fracture classification systems based on their ability to pair with regimens of treatment. By using the ETL, we hope to give surgeons a quick and efficient way to gauge the Sanders classification, which will provide them with reliable prognostic insight regarding the outcomes of patients with calcaneal fractures.
ConclusionOur study demonstrates that the ETL is a reproducible radiographic parameter that can be reliably used to predict between Sanders type I or II (ETL is “above”) and Sanders type III or IV (ETL is “below”) calcaneal fractures as well as the presence of lateral wall blowout. This radiographic parameter has the potential to increase efficiency in preoperative assessment as well as guide treatment of calcaneal fractures.
References 1. Sanders R: Displaced intra-articular fractures of the calcaneus. J Bone Joint Surg Am 2000;82:225-250. 2. Sanders R, Fortin P, DiPasquale T, Walling A: Operative treatment in 120 displaced intraarticular calcaneal fractures. Results using a prognostic computed tomography scan classification. Clin Orthop Relat Res 1993;290:87-95. 3. Gonzalez TA, Lucas RC, Miller TJ, Gitajn IL, Zurakowski D, Kwon JY: Posterior facet settling and changes in Bohler's angle in operatively and nonoperatively treated calcaneus fractures. Foot Ankle Int 2015;36:1297-1309. 4. Backes M, Dorr MC, Luitse JSK, Goslings JC, Schepers T: Predicting loss of height in surgically treated displaced intra-articular fractures of the calcaneus. Int Orthop 2016;40:513-518. 5. Touissaint RJ, Gitajn L, Kwon J: Measuring Bohler's angle with oblique lateral radiographs: Implications for management of calcaneal fractures. Harv Orthop J 2013;15:7-12. 6. Willauer P, Sangeorzan BJ, Whittaker EC, Shofer JB, Ledoux WR: The sensitivity of standard radiographic foot measures to misalignment. Foot Ankle Int 2014;35:1334-1340. 7. Isaacs JD, Baba M, Huang P, et al.: The diagnostic accuracy of Böhler’s angle in fractures of the calcaneus. J Emerg Med 2013;45:879-884. 8. Sayed-Noor AS, Agren P-H, Wretenberg P: Interobserver reliability and intraobserver reproducibility of three radiological classification systems for intra-articular calcaneal fractures. Foot Ankle Int 2011;32:861-866. 9. Loucks C, Buckley R: Bohler's angle: Correlation with outcome in displaced intra-articular calcaneal fractures. J Orthop Trauma 1999;13:554-558. 10. Hordyk PJ, Fuerbringer BA, Roukis TS: Clinical management of acute, closed displaced intra-articular calcaneal fractures. Clin Podiatr Med Surg 2019;36:163-171. 11. Daftary A, Haims AH, Baumgaertner MR: Fractures of the calcaneus: A review with emphasis on CT. Radiographics 2005;25:1215-1226. 12. Swords MP, Alton TB, Holt S, Sangeorzan BJ, Shank JR, Benirschke SK: Prognostic value of computed tomography classification systems for intra-articular calcaneus fractures. Foot Ankle Int 2014;35:975-980. 13. Bujang MA, Baharum N: A simplified guide to determination of sample size requirements for estimating the value of intraclass correlation coefficient: A review. Arch Orofac Sci 2017;12:1-11. 14. Piovesana LG, Lopes HC, Pacca DM, Ninomiya AF, Dinato MCME, Pagnano RG: Assessment of reproducibility of sanders classification for calcaneal fractures. Acta Ortop Bras 2016;24:90-93. 15. Schepers T, Van Lieshout EMM, Ginai AZ, Mulder PGH, Heetveld MJ, Patka P: Calcaneal fracture classification: A comparative study. J Foot Ankle Surg 2009;48:156-162. 16. Bernstein J, Monaghan BA, Silber JS, DeLong WG: Taxonomy and treatment – a classification of fracture classifications. J Bone Joint Surg Br 1997;79-B:706-707.
Comments (0)