Background
Hypertension is a major driver of healthcare costs. Remote physiologic monitoring (RPM) combined with team-based chronic disease care management can improve blood pressure (BP) control and reduce risk of high-cost cardiovascular events.
Objective
To examine whether a pharmacist-led Digital Medicine program improves BP control, medication adherence, healthcare utilization, and cost of care among racial subpopulations of Medicare patients.
Design
Retrospective single-institution observational study conducted between January 1, 2019, and October 15, 2023.
Participants
Medicare patients with hypertension enrolled in the intervention with ≥ 3 office-based BP readings within 6-month periods pre- and post-index event and their propensity score–matched controls.
Intervention
Remote pharmacist-physician collaborative care employing RPM with lifestyle, medication, and care gap management.
Main Measures
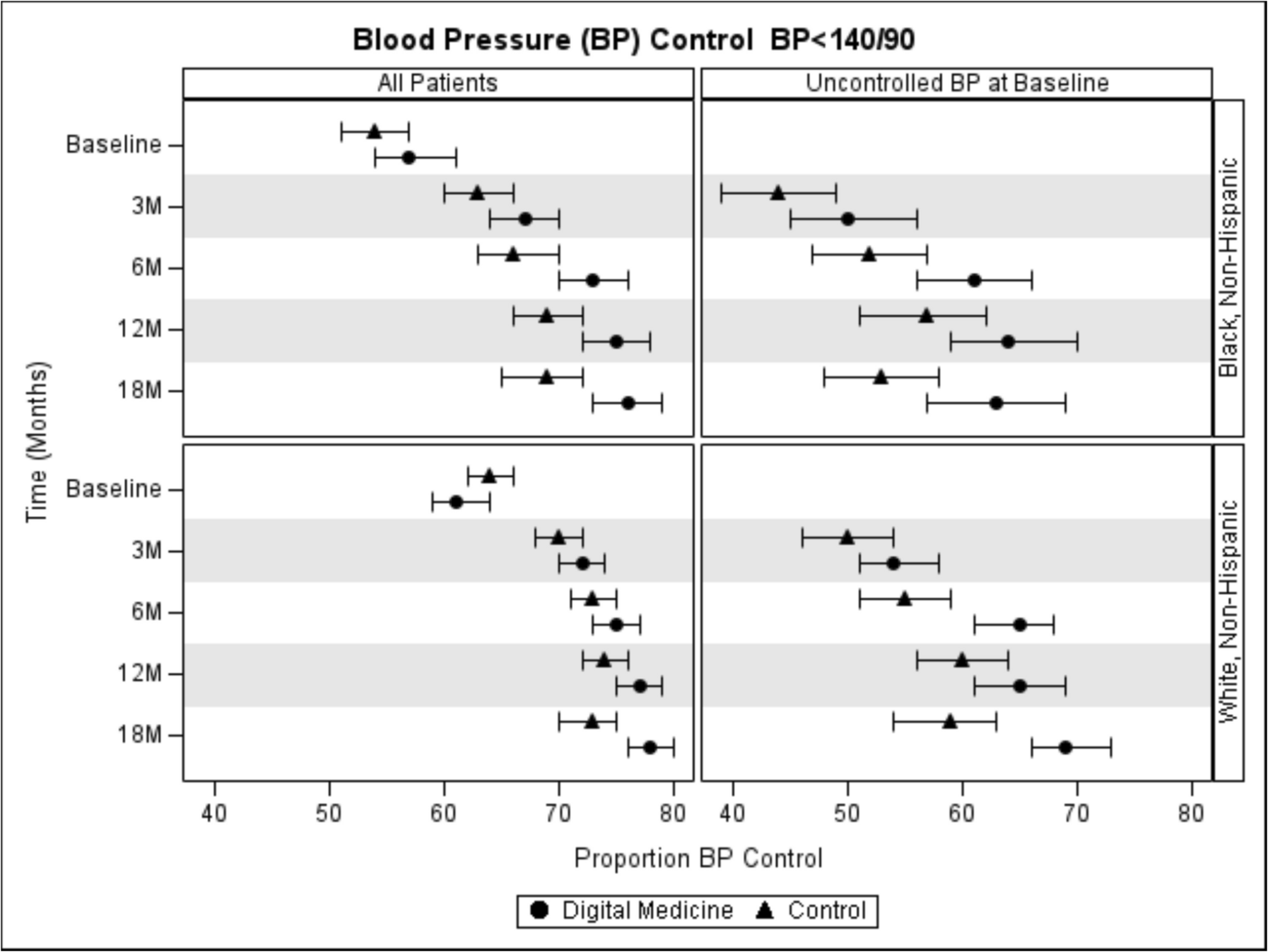
Primary outcome was BP control (office-based). Secondary outcomes were medication adherence, service utilization, and cost of care. Outcomes were assessed at baseline, 3, 6, 12, and 18 months using difference-in-difference (DID) approach stratified by race.
Key Results
A total of 5057 patients were included in the analysis. At baseline, Black patients had lower proportions of BP control. By 18 months, intervention compared to controls had higher rates of BP control (Digital-Medicine vs control, Proportion [95%CI]: Black, 0.761[0.728, 0.795] vs. 0.687 [0.654, 0.721]; White, 0.777 [0.755, 0.799] vs. 0.727 [0.704, 0.750]) and greater reductions in average SBP (DID, mmHg [95%CI]: Black, − 1.74 [− 3.18, − 0.29]; White, − 3.22 [− 4.22, − 2.23]) across racial subgroups. Differences in average DBP reductions were only significant for White patients (DID: Black, − 0.45 [− 1.23, 0.32]; White, − 1.48 [− 2.02, − 0.95]). Intervention compared to controls had higher odds of medication adherence, lower rates of inpatient and emergency department utilization, and no significant changes in primary care visits. Minimal changes in cost were observed.
Conclusion
Remote pharmacist-led care management increased BP control across racial subpopulations and improved medication adherence and acute care service utilization.



Comments (0)