Mood on Track (MoT) is a psychological intervention programme which combines group CBT for Bipolar Disorder and individual relapse prevention or ‘staying well’ work. MoT had been previously delivered solely in face-to-face format with promising outcomes demonstrated [17]. However, the present study aimed to investigate both the feasibility and acceptability of delivering Mood on Track online as well as establishing the feasibility of completing a future trial of online MoT efficacy.
The results of the current study suggest that digital delivery of Mood on Track is acceptable to service users attending a routine clinical service. Eighty two people began the Mood on Track programme and 74.39% of these attended 10 or more group sessions which would be considered a dose of group CBT as they covered the vast majority of the intervention content. The average number of group sessions attended was 10 of 13 which would be considered a high attendance rate for a psychological therapy. Subsequently, the majority of those who completed the group element of the programme (79%) went on to receive individual staying well sessions to create their own staying well self-management plan. This suggests the intervention was acceptable to service users, treatment adherence is likely, and the intervention is appropriate for a larger study. Qualitative data will be reported elsewhere which supports the acceptability of the group intervention.
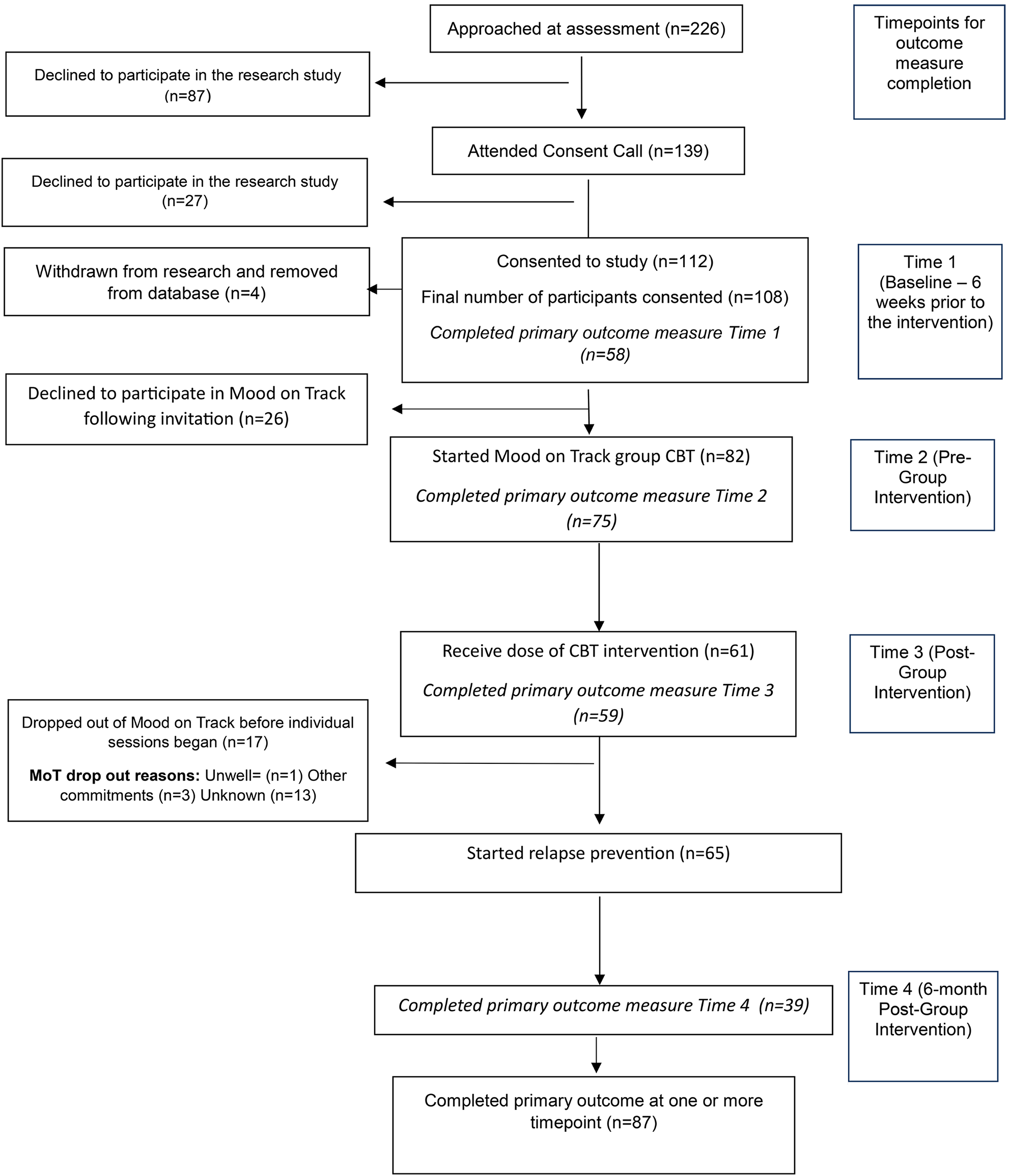
Furthermore, the recruitment rate to the study was positive with 112 of 226 (50%) of people approached giving consent to participate in the research study from all referrals to the clinical service during the recruitment period. In this pragmatic study service users referred to the team and assessed as suitable for Mood on Track were offered the intervention, regardless of their participation in the research study. Therefore, for some participants it is likely there was less incentive to take part in the study because they were still offered the intervention even if they declined to participate in research. As such, the recruitment rate for the study must be interpreted differently to the offer acceptance rate of Mood on Track. Although there was no element of randomisation in the current study, this shows a positive signal that potential participants will be interested and willing to consent to a future planned research trial of Mood on Track online. Overall, recruitment numbers within the study confirm that it is feasible to recruit participants and suggests that recruitment into a larger-scale study would be feasible.
Completion rate for the primary outcome measure was between 44.83% and 86.21%. Although the rates were variable at each timepoint, they suggest that participants can complete self-report measures on a regular basis and that a future study would garner sufficient outcome measures to evaluate the intervention on a larger scale. The increase in completion from Time 1 baseline (58 participants) to Time 2 pre-group intervention (75 participants) was due to the fact that at the beginning of each new programme some service users did not respond to their invitation to attend and others cannot or no longer wish to attend. Therefore, additional people were invited to take up the remaining vacant places. Unfortunately, this was after the 6-week baseline data had been collected and therefore, for these participants, no baseline data was collected impacting the data available in the analysis. This scenario would be avoided in a future randomised control trial, in which a deadline for inclusion and completion of baseline measures would be set (unlike the current pragmatic clinical design in which service users could still join the group having missed the initial baseline measure). Therefore, participation would require completion of the baseline measure prior to inclusion, and this would improve data quality.
Although there was adequate data completion to conduct an analysis of efficacy, there was a drop in outcome measure completion at the six months follow-up. This lower rate of completion was likely because service users had completed the intervention and therefore been discharged from the clinical service, with no further planned contact. Therefore, it was more challenging to encourage people to complete the measures. Additional assertive follow up strategies would need to be implemented in a future trial.
Another reason for outcome data loss was due to drop out from the clinical intervention (either before or after the first week), however this rate of drop out aligns with clinical expectations. Overall, despite the lower completion rates at baseline and follow-up, completion rates at all timepoints were satisfactory to complete data analysis and thus indicate feasibility for a future larger-scale study.
In addition to demonstrating feasibility and acceptability of people engaging in Mood on Track and of conducting a future study of online psychological interventions for those with bipolar disorder, the quantitative findings described show promising signs of efficacy. For the primary outcome there was significantly increased self-reported recovery between the start and end of group, as well as further significant increases six months after completion. Anxiety scores also significantly reduced between the start and end of group, and this was maintained at follow-up. There were some indications that depression, work and social adjustment and quality of life improved but that changes in these areas began whilst people were waiting for the group to commence so although the changes continued in a positive direction this cannot be said to be over and above what we could expect should this baseline change continue. This is often the case with wait list control designs. Participants can begin to feel better when they wait for the intervention as they may feel hopeful that they will recover. Some of these effects may be better understood by comparing treatment with a control group in a Randomised Control Trial. Given the significant positive changes reported in this study we would suggest that the main outcome measure of bipolar recovery (BRQ) should be used in a future randomised controlled trial and that measuring anxiety, quality of life, work and social adjustment and depression would also be important to consider as secondary outcomes.
Furthermore, interventions such as Mood on Track could be helpful in reducing relapse and consequently suicide risk as they allow service users the opportunity to explore making lifestyle changes as well as managing stressors that may previously have led to mood change. It would be beneficial to study this in future longitudinal research. The intervention aims to help people to identify early signs of mood change and to ask for help if needed, prior to a crisis occurring. Longer term outcomes of the intervention such as relapse rates and crisis use should be further investigated in any future research.
The reported findings suggest that digital delivery of psychological interventions for BD hold promise for both services and service users and support previous studies which found positive clinical change following online intervention [18,19,20]. When effective, group CBT online is also cost-effective because two therapists can see fifteen service users at one time from their home or office base. Service users from a wide geographical area can be seen without the need for travel by either service user or staff member. Those with bipolar disorder can face challenges with attendance and mood change which can make engagement in therapy problematic. Digital delivery has the potential to increase inclusion and overcome some of these barriers [36] and could be particularly helpful for those with a diagnosis of bipolar disorder.
Strengths, limitations and future investigation
The service user steering group was a strength. This group was instrumental in advising on data collection procedures which likely contributed to increasing outcome measure completion rates. For example, an increased uptake in completion of follow up data was noted following the implementation of a suggestion to send a reminder postcard to participants thanking them for participation to date and reminding them that the final questionnaires would be sent to them in a few weeks’ time.
The use of a six-week pre-group baseline measure provided a treatment-as-usual comparison for the outcome measures completed during the intervention stage. Although participants may have found this an extra burden, the completion rates were sufficient for an initial analysis of efficacy to be conducted and suggest they are feasible and acceptable for participants to complete in a larger future trial.
The procedure for the analysis of efficacy used both a per-protocol and completer analysis, which allowed all of the collected data to used despite gaps due to non-completion. Furthermore, using Scheffé’s method allowed for multiple t-test comparisons to be made whilst still controlling for the familywise error rate. However, as the study was designed to assess feasibility and acceptability, a power calculation was not completed and therefore, the results must be interpreted carefully and can be viewed as sufficient evidence to warrant a larger scale trial with a powered analysis. Furthermore, a larger scale study could be designed as a randomised control trial. The present study was non-randomised and therefore, there could have been a self-selection bias from service users. However, a non-randomised design was used because this study was designed to assess feasibility and acceptability. Now that this has been established, there is a rationale for randomising a future trial.
The present study is unfunded and took place within a busy NHS clinical service for people with bipolar disorder. A larger funded follow-up study would allow for improvements in data collection e.g. the presence of research staff to prompt participants to complete outcome measures, particularly at the six-month timepoint. Furthermore, in a future study the reasons for declining participation and dropping out of the intervention could be recorded in more detail.
Given that depression and hypomania fluctuate across time for those with bipolar disorder, perhaps an alternative way of studying whether the intervention impacts depressive and hypomanic episodes following the intervention is to consider periods spent in depression or hypomania over time and by measuring relapse, hospitalisations and utilisation of home-treatment and crisis services, rather than comparing depression or hypomania over the treatment period and follow up.
Despite the limitations discussed and remaining cautious in our interpretations, when the present study is taken together with other existing research studies, the findings from this study provide further promising evidence that online psychological interventions can lead to improved wellbeing and mood for service users with Bipolar Disorder [18,19,20,21,22]. We believe this to be one of the first online psychological therapy studies for this specific population. Despite some of the concerns about providing psychological therapy online noted in the introduction [25] and the practical and therapeutic challenges of providing group CBT online, this study provides initial evidence that this is a feasible and acceptable intervention for those with a diagnosis of bipolar disorder and one that might significantly aid their recovery.
In the UK, NICE guidelines suggest that psychoeducation, CBT and relapse prevention work are all important for people with bipolar disorder. Mood on Track includes all three of these elements, and the inclusion of relapse prevention planning can be hypothesised to explain why there were further significant increases in recovery scores at follow-up after group CBT. Therefore, our overall hypothesis is that the Mood on Track programme in sum may be better than each of its elements. A future study could help to further understand what changes may be related to the Group CBT component, what changes can be attributed to the relapse prevention component and whether it is beneficial to provide these in combination.



Comments (0)