User fees as a mechanism of cost recovery in developing countries were advocated by the World Bank (WB) in 1985. Since then, user fees were implemented in many low- and middle-income countries with the support of the World Bank and the World Health Organization (WHO) [24]. Supporters of user fees hypothesize that those fees are a sustainable source of funding health services, especially in low-resource countries. In addition, those fees help improve the quality of provided services and reduce the inappropriate use of those services [1].
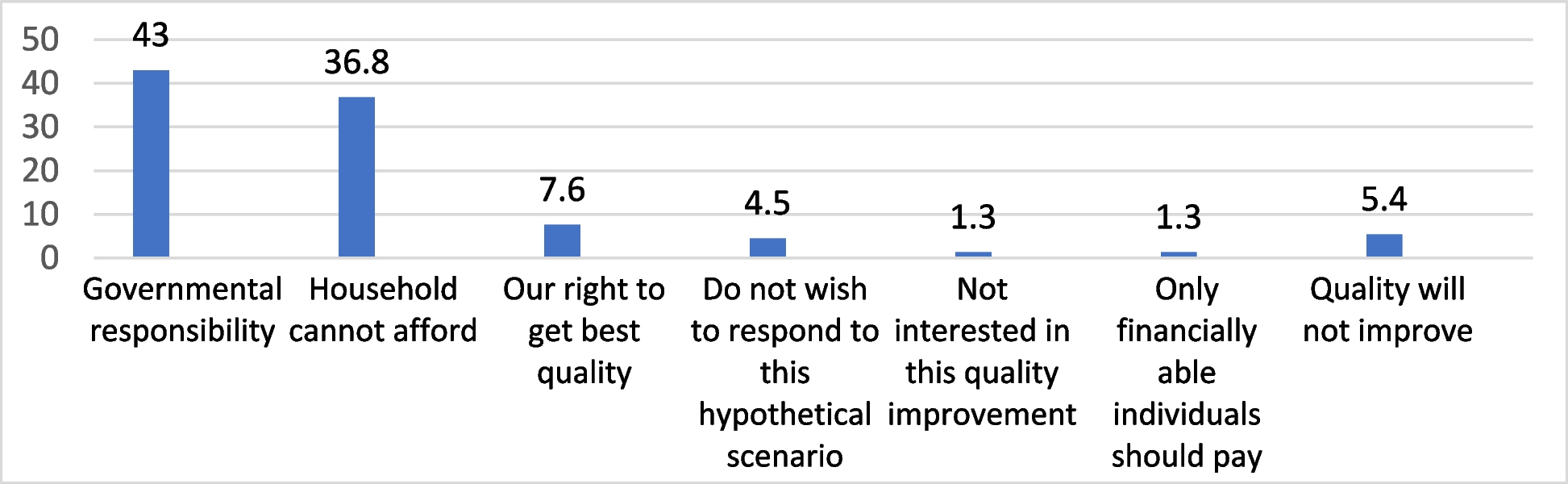
The current study aims to assess patients’ WTP for healthcare quality improvement in two hospitals in Egypt. The results revealed that almost half of the patients were not willing to pay for an improvement in the quality of health services. When asked about the certainty of willingness to pay, around half of those willing to pay reported that they were not certain of their willingness. For those who were not willing to pay, around half attributed this to healthcare being the government’s responsibility, and around one-third were unable to afford to pay for quality improvement. The quality attributes for which patients were willing to pay the highest amount were the doctor’s competence, outcomes, and doctor-patient relationship. For all quality attributes, with the exception of waiting time and availability of supplies and equipment, the amount of money the patients were willing to pay increased significantly as the perceived quality of that attribute reduced.
4.1 WTP and its policy implications
The WTP in the current study was lower than that reported in other studies. In 2001 in Sudan, a household WTP survey revealed that 80% of those paying a charge for the health services and 75% for those receiving it free of charge were willing to pay for quality improvements of health services [3]. In Palestine in the period from 2001 to 2003, WTP to improve the quality of health services in primary care units dropped from 78.0% in 2001 to 61.0% in 2003 [25]. In another study conducted among attendants of primary healthcare centers in Palestine, 93.4% declared they were willing to pay higher user fees to benefit from better quality [4]. In a national survey conducted in the Central African Republic, WTP ranged from 64.0% to 81.0% for seven quality attributes for improving child care [26]. In a household survey conducted in 2000, the majority of Bulgarians were in favor of paying for public services with good quality and quick access [27].
The low results of WTP in the current study can have several explanations. One of the explanations is that the current study utilized a PS in eliciting the WTP compared to the closed-ended format used in the Central African Republic and Sudan studies and the dichotomous choice in the Palestinian study [3, 25, 26]. Closed-ended WTP format resulted in significantly higher valuations than the PS formats in a study eliciting the WTP for alternative methods of screening for colorectal cancer [29]. Similarly, the dichotomous choice format has been shown to consistently generate larger values than the PS [28, 29].
Another explanation for the low percentage of respondents willing to pay in the current study is the high level of inflation and the tightening financial conditions in Egypt since the devaluation of the Egyptian pound in March 2022. This resulted in an increase in poverty rates [30, 31]. The GDP per capita in Egypt is US $3457 which places Egypt in the 92nd rank compared to other countries. In their study, Mataria et al. demonstrated that WTP for the attributes geographical proximity and waiting time were most affected by the substantial reduction in patients’ income. This can be explained by the fact that quality attributes perceived to be nonessential luxuries are significantly affected by income reduction. On the other hand, the WTP for essential quality attributes such as drug availability and doctor-patient relationship were not affected by impoverishment [25]. Similarly, in the current study, patients were willing to pay the highest amount of money to improve the quality of the attributes “competence,” followed by “outcome” and “doctor-patient relationship.”
In the current study, household head income was not significantly associated with WTP as opposed to health expenditure. This was explained by Russel as the difference between WTP and ability to pay (ATP) [33]. He proposed that households may cope with the user fees for healthcare by sacrificing other basic needs such as food and education or by borrowing and selling assets. According to the Egyptian Health Insurance law, user fees upon receiving service will be applied but with an exemption for those unable to pay [34]. However, there is no explicit mechanism for defining those who are unable to pay [19]. Thus, national “inability to pay” income criteria should be clearly defined against which people will be judged for exemption. In addition, further research on the mechanisms the patients use to cope with healthcare costs should be conducted.
A third explanation for the low level of WTP is the level of trust in the government in Egypt. According to a report by the Arab Barometer in 2019, 66% of Egyptians reported having a great deal or quite a lot of trust in the government [35]. In another report by the European Bank for Reconstruction and Development, corruption was still perceived as a problem in public and private organizations [36]. In research analyzing data from the fifth wave of the Arab Barometer survey to identify the main determinants of public trust in the government of Egypt, perceiving national institutions as corrupt had a negative impact on the likelihood of trusting the government [37]. In a survey covering 29,526 respondents from 29 countries, an increase in social trust was associated with a greater WTP for more taxes to improve public healthcare [38].
In the current study, around half of the respondents believed that improving the quality of healthcare is the responsibility of the government and not the citizens. Thus, building social trust in the government as well as the health system is a cornerstone for the public to share in funding the healthcare system. According to Gilson, trust in the healthcare system can be built through fairness in the distribution of health resources by ensuring geographical, financial, and cultural accessibility for all and through setting equality goals [39].
In the current study, the percentage of those willing to pay decreased significantly as age advanced and the level of education decreased. Similar findings were reported by Mataria et al. among patients attending primary care units in Palestine and by Al-Hanawi et al. among heads of households in Saudi Arabia [4, 5]. In a systematic review of determinants of WTP for health services, age was a significant determinant for WTP in 30 out of 50 studies, whereas education was a significant predictor in 30 out of 45 studies (60.0% and 66.7%, respectively) [15]. In another review assessing the WTP for national health insurance services in Asia and Africa, the age of the household head was significantly and negatively associated with WTP in 7 out of 19 studies, and education was significantly and positively associated with WTP in 5 out of 19 studies [40].
One of the explanations for this finding is that as people age, their income decreases, resulting in a reduction in their capacity to pay for health services [41]. Although this study did not attempt to measure demand elasticity, we could expect that the demand is elastic among the older population and those with lower education, which could result in a reduction in accessibility among those groups. If policymakers are aiming at equitable accessibility among different population groups, a price discrimination approach should be adopted if user fees are used to co-fund the quality improvements in health services [4, 42]. According to the results of our study, lower user fees should be charged to the elderly and those with lower education attainment. In addition, the government should subsidize the care for price-sensitive groups of the population and closely monitor how the level of demand was affected by the introduction of user fees [43].
The mean value the patients were willing to pay increased significantly as the patients’ ratings for the attributes distance from the hospital, physicians’ competence, hospital cleanliness, and quietness decreased. For example, patients who rated the hospital as “very far” were willing to pay three times as much as those who rated the hospital as “very close.” Similarly, in the logistic regression model, those who rated the hospital as “very far” had 3.7 higher odds of WTP for receiving care compared to those who rated the hospital as “very close.” This finding was similar to those reported in Saudi Arabia and Bangladesh where WTP and the amount of money the patients were willing to pay were inversely related to the rating of different quality attributes [5, 12]. This would be a validation of the WTP methodology used as patients were willing to pay to improve attributes with low-perceived quality. In the current study, we assumed independence between different quality attributes. That is, improvement in one attribute is independent of the improvements over others. Further research should verify the existence of this independence.
4.2 Validity of the results of the contingent valuation methodology
The validity of the contingent valuation methodology has been widely questioned. The contingent valuation methodology in our study has been conducted during a time of economic recession in Egypt. Under tough economic conditions, people may modify their preferences to accommodate only services they consider “essential.” Thus, under those conditions, unwillingness to pay for quality improvement of certain service attributes should not be directly interpreted as a lack of preference for those attributes [4]. Economic and social conditions should be considered when interpreting the results of WTP surveys.
Our study attempted to improve the validity of the WTP survey through several techniques. First, to reduce the “hypothetical bias” which is the extent to which the WTP scenario and the valuation task are believable by the respondents [22], the valuation scenario in the current study was insurance based (i.e., insurance premium) rather than a user-based scenario (i.e., user fees at the point of consumption). This approach made the scenario more realistic as the Universal Health Insurance Law was issued in 2018. Until the time of the study, it was piloted in several governorates [16]. The Egyptian Healthcare Authority is planning a phased implementation of the new universal health insurance system until universal health coverage encompasses all governorates by 2030. Thus, the insurance-based scenario was realistic and understandable for the respondents [44].
To reduce the respondents’ cognitive load and improve the accuracy of the results, the decomposed valuation scenario approach was employed instead of the holistic approach in which the respondents are asked for the monetary value for quality improvement in general [4]. O’Brien et al. recommended that if multiple attributes are to be valued, three or four most valuable ones should be identified. WTP exercise should be based on each attribute separately [5, 45].
The current study utilized the PS methodology for eliciting WTP values. Compared to other CV methods, the PS methodology avoids starting point bias inherent in the bidding game and dichotomous choice formats since the questions do not offer an initial bid. Also, it avoids the “yea-saying bias” in dichotomous choice surveys. PS also reduces the cognitive load on the respondents since they are offered a predefined set of values. On the other hand, PS entails a range bias, where the range of bids affects the valuation. Respondents may choose to report a comparatively higher WTP in a hypothetical exercise if their true WTP value is relatively low compared to the values displayed on the PS and vice versa [11, 46].
Respondents may be able to elicit values that are closer to their “true” WTP values if the range is more realistic. In our study, the range of values was piloted among several patients to ensure that it is realistic. In addition to selecting a valuation from the PS, respondents were asked to choose from the PS the amount they were definitely willing to pay (minimum WTP) and the amount they were definitely not willing to pay (maximum WTP) for each attribute. This was followed by an open-ended question to select a value between the minimum and the maximum WTP to further reduce the range bias.
To predict the actual consumption behavior, a post-estimation response certainty question was asked. Respondents were asked how certain they were about paying for the improvement of different quality attributes if they were asked right now. Among those willing to pay in our study, only half of the respondents were completely certain they were willing to pay. Four-fifths of those willing to pay were private hospital respondents, and one-fifth were insurance hospital respondents. This could be an indication of the respondent’s actual behavior in real situations where the WTP percentage would be much lower than that reported, and we can even expect the monetary values to be lower [34].
4.3 Limitations of the study
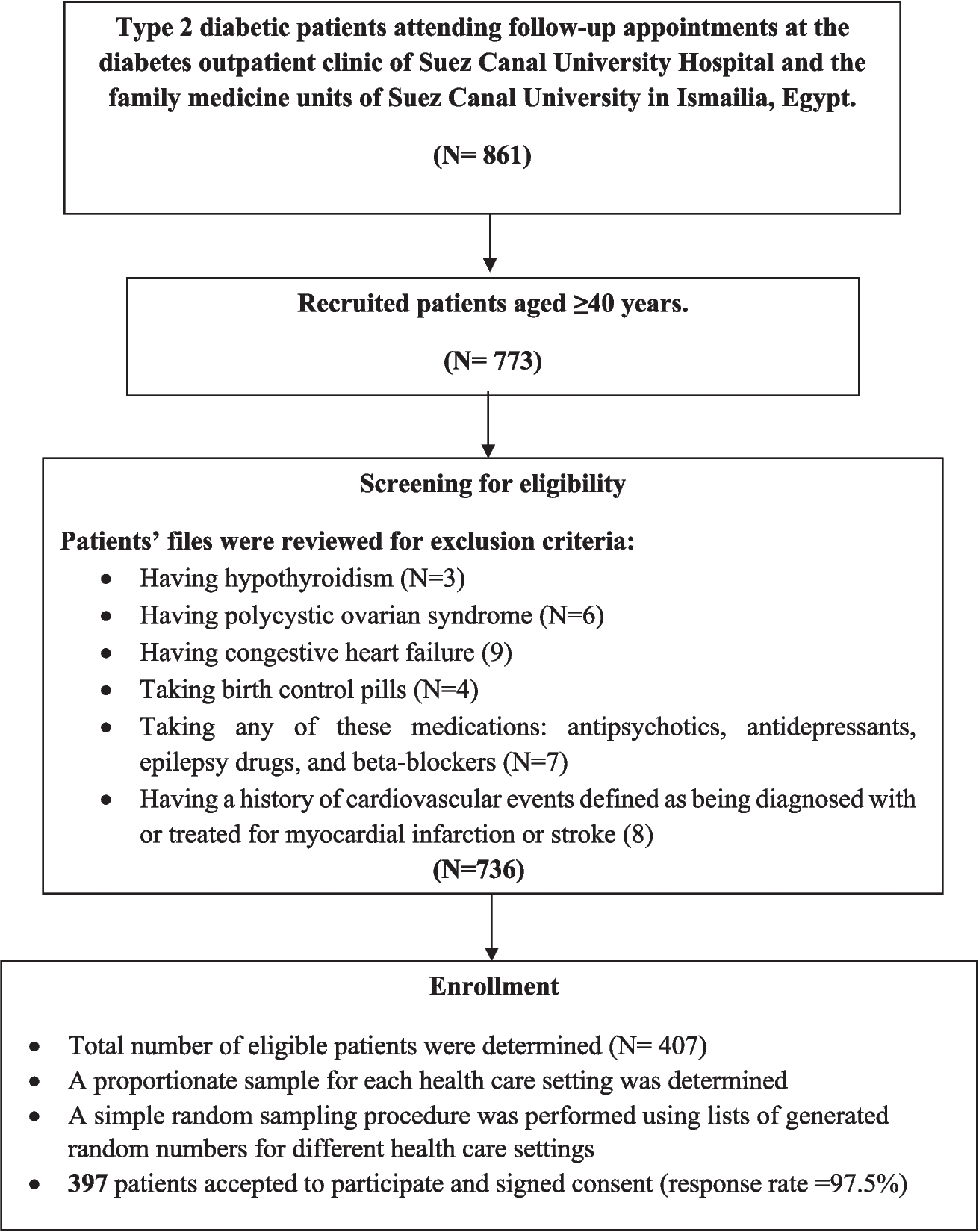
Despite being the first study to measure WTP among the Egyptian population, the current study has selected an “in-site” sample rather than a household survey. Thus, those who did not attend the healthcare facilities were not represented. Moreover, not all facilities were represented as, for example, patients attending the Ministry of Health and University healthcare facilities were not included. Those groups are usually socially and economically disadvantaged compared to patients currently covered by the social health insurance system or attending private facilities and paying out of pocket. Further research should be conducted covering wider segments of the population and using household surveys.


Comments (0)