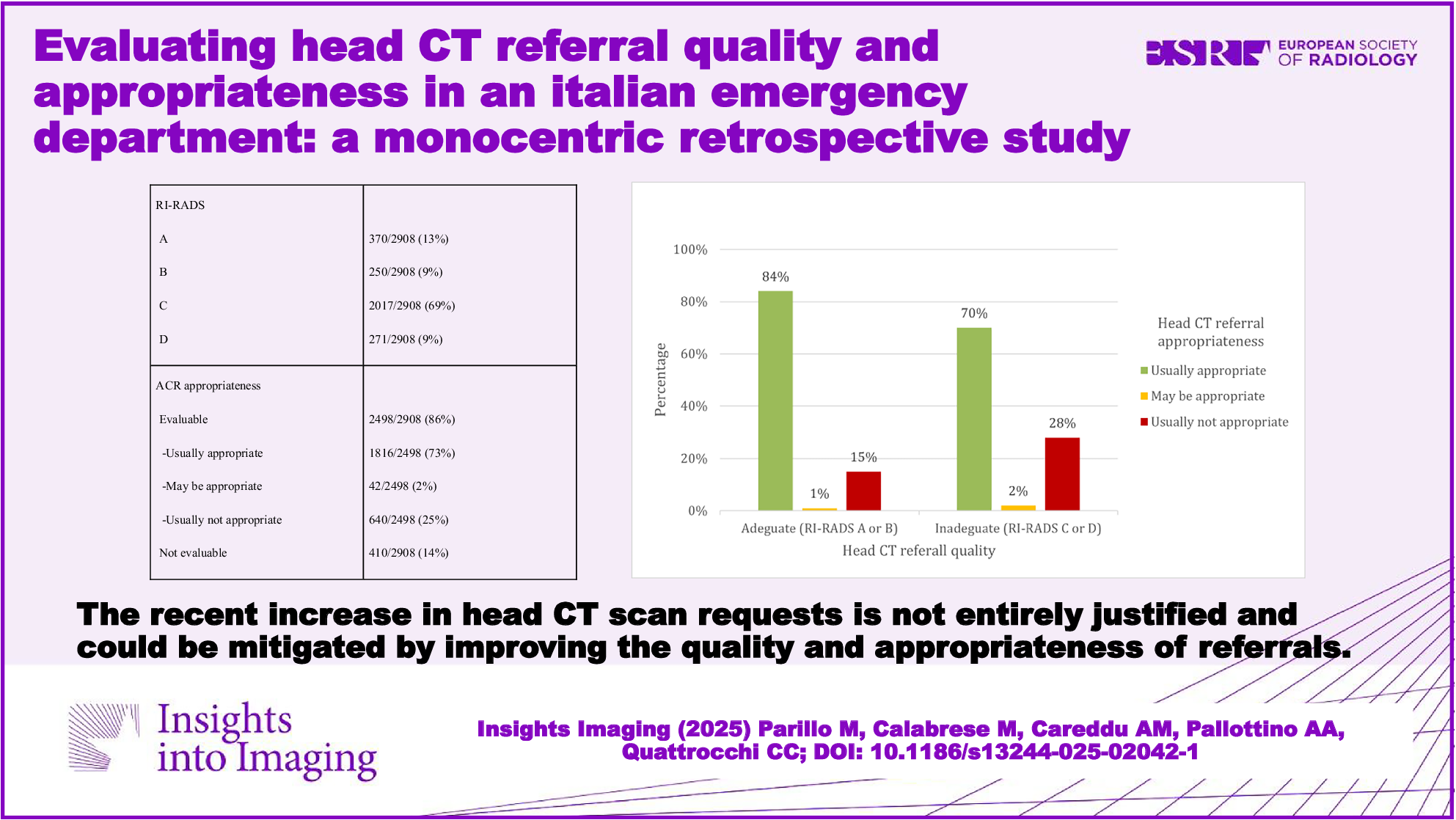
This study shows that the majority of unenhanced head CT requests in the ED were inadequate in terms of quality (79%), especially when a specific diagnostic question is missing, with a high rate of inappropriateness in terms of clinical indication (25% considering only the referrals that could be correctly evaluated). The risk of inappropriate head CT scans could be mitigated by improving the quality of requests, as suggested by the lower number of appropriate requests scored as RI-RADS C or D. This can be attributed to the difficulty emergency physicians face in applying guidelines without a clear diagnostic query. Furthermore, defensive medicine, which is widespread but especially prevalent in emergency settings, plays a significant role, with CTs often requested under the false assumption of improved legal standing.
Headache and syncope, accounting for roughly half of all inappropriate requests, were identified as the leading clinical indications for inappropriateness. This highlights the necessity for enhanced training and education on appropriate CT utilization, particularly in these clinical situations.
Moreover, appropriate indication was associated with a higher likelihood of identifying cerebral findings and, considering the most frequent clinical indications, showed a high predictive value for the actual presence of an acute cerebral pathology on radiological examination. This reinforces the notion that the recent increase in head CT scan requests in the ED is not justified. Inappropriate CT procedures represent an unnecessary expense in economic, environmental, and unjustified radiation exposure terms. In particular, the issue of radiation exposure has received considerable attention nowadays, exemplified by the 2013/59/EURATOM directive outlining basic safety measures for protection from ionizing radiation hazards [29], which Italy implemented via Legislative Decree 101/2020 [30]. According to Article 159 of the decree, the radiologist is the professional who bears primary responsibility for evaluating the appropriateness of radiological examinations, including CT scans. Ideally, the process of requesting a radiological examination begins with a motivated request from the referring physician (prescribing physician), which highlights the clinical necessity of the examination. The radiologist then evaluates this request, taking into account the clinical information provided, the suitability of the requested examination to answer the clinical question, and the possibility of using alternative imaging modalities that involve lower radiation exposure. The radiographer also plays an important role in verifying the consistency between the clinical question and the prescription and can report cases that do not generally appear justified to the radiologist for further evaluation. Although this workflow is desirable, it is often difficult to apply in daily clinical practice, especially in the emergency setting, when refusing to perform a radiological examination based on the aforementioned dictates could, although rarely, lead to significant clinical consequences for the patient. Furthermore, the daily heavy workload makes a detailed evaluation of all radiological requests difficult for a single radiologist, and radiographers cannot be sufficiently trained to assess appropriateness in all cases.
Previous studies have partially examined this topic. Ferorelli et al examined 100 head CT requests originating from the ED. Appropriateness was assessed retrospectively and blindly by a panel of expert radiologists, neurologists, and anesthesiologists. The results indicated that 32% of the CT examinations were deemed inappropriate, with 6% of these attributed to defensive medical practices [8]. A retrospective analysis by Nishtar et al examined all head CT scans conducted at an ED within a Pakistani hub center from November 1, 2017, to January 31, 2018. The analysis of 3893 scans revealed a 33.7% positivity rate, with the majority of positive findings related to major trauma or neurological deficits in elderly patients. The study argued for CT overuse, resulting in increased costs and radiation exposure, but its conclusions were drawn solely from positivity rates, without evaluating appropriateness [7]. The Ethiopian study by Demeke and Mekonnen aimed to identify the extent of inappropriate cranial CTs by evaluating all CTs performed during a given period in the radiology department of a specialized hospital, including both emergency/urgent and scheduled CTs. It considered only requests with a complete or almost complete set of the required information (> 80% of the information). The final sample comprised 443 CTs. The appropriateness was evaluated according to the ACR guidelines: 51.9% fell into the “usually appropriate” category, 15.1% were considered “possibly appropriate.”, and 11.7% were deemed inappropriate. In the remaining 21.3%, the requests did not fit into any of the ACR criteria categories. Headaches (38.5%), seizures (23.1%), and head trauma (23.1%) were the most common indications for inappropriate scans [9]. Employing the same ACR guidelines, this Ethiopian study offers a relevant comparison to our findings, though it included both emergency and scheduled CT examinations. Our methodology, which involves evaluating request quality prior to appropriateness assessment, is supported by the authors’ emphasis on the critical need for thorough imaging requests to convey clinical justification. To standardize the imaging referrals quality evaluation, we used the RI-RADS categories [15, 16]. This system enables radiologists to evaluate the completeness of provided information and communicate this assessment in reports. By incorporating RI-RADS ratings, radiologists furnish feedback to requesting physicians, creating a “rating sheet” that promotes the provision of accurate and comprehensive clinical details [17]. Initially, we planned to assess appropriateness solely for requests rated adequate by RI-RADS (A or B). However, a shortage of adequate requests, primarily due to missing diagnostic questions, necessitated expanding our evaluation to include inadequate requests (RI-RADS C or D) where appropriateness could still be determined from available data. Evaluating inadequate requests for appropriateness introduced a potential bias: the data collectors’ assessments might have been skewed due to the absence of crucial clinical details, potentially masking diverse clinical presentations. For example, a headache request lacking “red flag” information could lead to inaccurate appropriateness judgments. On the other hand, the inclusion of inadequate requests proved important for the methodology, as these CT examinations were indeed performed and therefore offer insights into quality improvement.
To increase the level of quality and appropriateness of radiological requests, it is important on the one hand to integrate guidelines into clinical workflows and decision support systems within electronic health records, and on the other hand to implement robust mechanisms for the prospective justification of radiological examinations, ensuring that the rationale for each examination is clearly documented in the patient’s medical record. By requiring specific signs, symptoms, or diagnostic queries before submission, such a system would necessitate physicians completing a structured questionnaire with predefined answers (e.g., present/absent, duration). This would minimize radiologist misinterpretation and facilitate the retrieval of precise clinical data. To increase the level of appropriateness of head CT requests, one option would be to develop educational programs sharing the ACR criteria with the ED. Another option to increase confidence in appropriateness would require making the emergency team aware of the ESR iGuide as an accessible and trustworthy resource for requesting physicians.
Moreover, the use of artificial intelligence, particularly through the text analysis of large language models (LLMs) [31], presents a promising avenue for influencing imaging referral evaluations. Physicians could input their radiology requests into the hospital’s electronic system and receive immediate feedback on RI-RADS grading or ACR appropriateness, allowing for real-time adjustments to request completeness. The validity of using various LLMs as a tool for evaluating the quality and appropriateness of radiology exam requests across a range of clinical cases is a topic for future studies.
A careful interpretation of our study’s results is warranted, given several inherent limitations in addition to the previously mentioned potential bias related to the analysis of incomplete requests. It should be acknowledged that written radiology requests may not encompass the entirety of information shared by referring physicians, as supplementary details might be conveyed verbally. Nevertheless, complete written imaging requests are crucial to reduce the risk of errors and miscommunication. Due to its single-center design and the focus on head CT examination, the study’s conclusions may not be universally applicable. The exclusive inclusion of ED patients limits the applicability of our findings to other patient populations, such as those in outpatient or inpatient settings. Furthermore, the heterogeneous nature of our patient cohort complicates direct comparisons with other clinical contexts. Conversely, the consecutive enrollment of imaging referrals ensured a realistic representation of the head CT demands faced by radiologists in emergency clinical practice. Finally, the potential impact of various factors on request completeness and appropriateness was not investigated in this study. For instance, future studies could assess whether the level of appropriateness and quality of radiological requests correlates with the referring physician’s clinical experience, to implement targeted educational pathways.






Comments (0)