Piloting and Evaluating Feasibility of the CTC Service
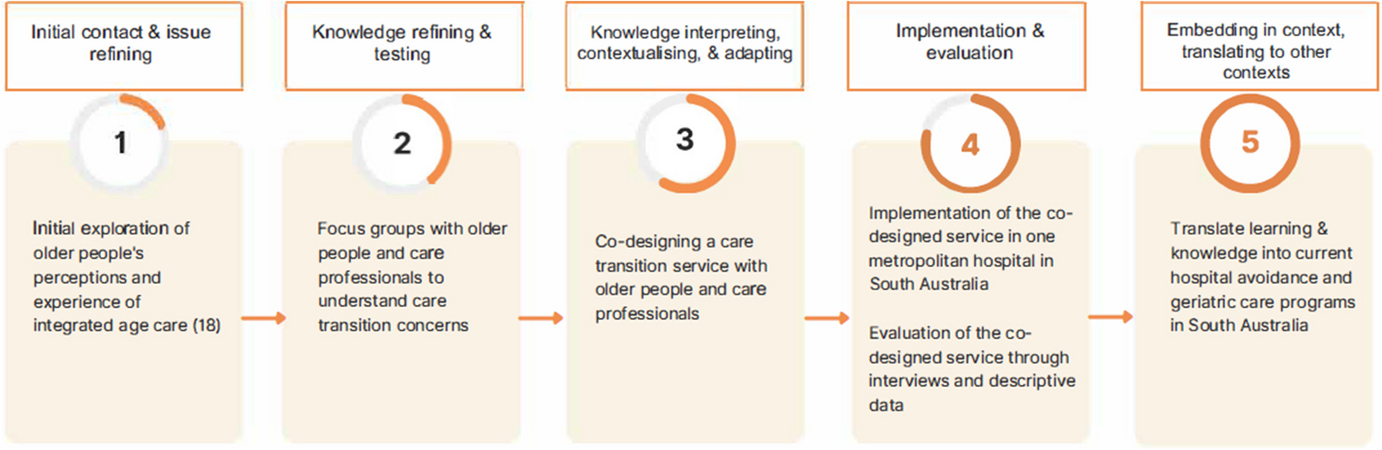
Following the five co-design workshops the final stage was to establish and pilot the CTC service and determine the feasibility of the service from various stakeholder perspectives. Although originally proposed as a role fulfilled by one health care professional to be based within the Geriatrics team at a metropolitan hospital, upon discussion with the Geriatrics team it was decided the role might be best performed by two people, to address both the clinical and social support needs identified by older people. Thus, the CTC service was established with a Clinical Nurse (CN), supported by an Allied Health Assistant (AHA) (collectively referred to as the CTC service hereafter). The co-designed CTC service was piloted for 6 months, from May to October 2021.
Client Demographics, Goals, and Participation
A total of 35 clients (21 female, 14 male), aged between 76 and 97 (mean age = 87) received care from the CTC. 16 clients declined the offer of the service. Reasons for declining the service included readmissions to hospital, a move to respite or residential aged care, or a view that they were already receiving sufficient support from family and formal carers.
The average duration of contact with the CTC service was 31 days, although there were some clients who had a shorter or longer period of interaction with the service. Unplanned admissions in the 6-months prior to receiving the CTC service ranged from 0–11 (mean = 1.5), compared to 0–7 (mean = 1.2) unplanned admissions in the 6-months post the CTC service.
Of the 35 clients, half (n = 15) had a Comprehensive Geriatric Assessment conducted by the CTC Clinical Nurse. These data indicated that most clients who completed the assessment shared similar goals of wanting to stay in their home with supports (73%), to improve their health through monitoring (47%) and to plan for the future and/or receive assistance with transport. Not all clients received a Comprehensive Geriatric Assessment, usually because one had already been completed, for example, while they were in hospital.
CTC Services Provided
Data extracted from service provider action sheets (n = 33) demonstrated that CTC services included home visits, phone calls to clients and their family/carers, and transport (for example to GP appointments, vaccination, pharmacy) (Table 4). The CTC also assisted with domestic duties including washing/cleaning and providing information about and connection to services such as Aged Care Assessments (ACAT), My Aged Care and Government funded Home Care Packages (Table 5).
Table 4 Activities Undertaken by the CTC ServiceTable 5 Description of Activities Undertaken by CTC ServiceThe majority (70%) of CTC activities were carried out by the CN, who had direct access to the ACAT team and was experienced in community geriatric care. The CN conducted medical checks including blood pressure monitoring and wound dressings, and liaised with all stakeholders, including clients and their families, referrers, medical staff, and aged care service providers. The CN also assisted with transport, shopping, cleaning, and client’s personal care and hygiene. The AHA carried out 23% of the CTC activities, liaising with clients, families, and stakeholders, conducting home visits, assisting with general household tasks, and providing clients with transport home, to the shops, GP appointments and pharmacy. The range of services provided by the CTC staff varied widely and was often beyond the scope of their traditional roles. To fulfil the requirements of the role, the CTC staff reported working additional hours beyond their allocated time – raising questions about the feasibility of the CTC service as a stand-alone provision carried out by a CN and an AHA.
Service Users, Providers, and Referrers Experience
Interviews were conducted with 3 service users (SU) (clients/family), 2 service providers (SP) (Clinical Nurse, Allied Health Assistant), and 4 referrers (RF) (Occupational Therapist, Geriatrician, Medical Officer, and Nurse Practitioner). Interviews ranged between 7 and 35 min in duration.
Eight parent codes were identified which related to the service users, providers and referrers to the service, living arrangements, client social life and goals and CTC service activities delivered. Key ‘child’ sub-codes that were common across stakeholder groups that address the aims of the pilot are described in the results section: navigating the aged care system, providing practical support, and supporting family/carers. Three additional themes were identified within the referrer/provider group: bridging the gap, building confidence, and providing eyes in the home.
Navigating the Aged Care System
Participation in the program helped clients and their family/carers navigate the complex aged care system, highlighting the services available to them. One of the principal activities the CTC service enacted was connecting clients and their family/carers with appropriate support services to help clients remain in their own homes. Clients and their families were not always aware of the services available and/or they were unsure how to access them. The aged care system was viewed as “really hard to navigate” (SP1) and having support with this was perceived as helpful.
You really do need someone to help you try and navigate the system. (SU1)
Even people who are capable of trying to navigate through struggle with it […] you can imagine the older person struggling to sort of organise the appointments. (RF2)
One referrer noted that they often referred clients for ACAT assessments, however they had no way of ensuring the patient engaged with the referral once discharged. The CTC service could help to bridge this gap.
Once the patient leaves the hospital, we can't really follow that up and so having that person there to kind of navigate all of that is actually beneficial. (RF1)
By helping clients connect with appropriate services the CTC service helped secure ongoing supports for clients to remain in their own homes.
Providing Practical Support
Clients often needed simple yet essential practical support, including ensuring they had enough food, medication, clean clothing, and clean and uncluttered homes to decrease the risk of falls. The CTC was able to provide this practical support including transport to the shops, pharmacy, and medical appointments.
We went there every day, did his washing, did his shopping, he could still cook meals to a degree. (SP2)
They were able to clear some of the clutter, to get her shopping, to get the food into the house and to do that basic work to get her out of hospital, there is no other service that does that at this time. (RF4)
She took me to the doctors, and actually went into the doctors and watched them dress my leg to make sure it was alright. (SU2)
The service was perceived as going “above and beyond” the provision of “minimal services” (SU1).
Supporting Families/Carers
In many cases, family were the main source of support for clients. The CTC service provided relief for family/carers in both the short term, by assisting with tasks the family usually performed, and in the long term, by helping families navigate the aged care system to secure ongoing support for daily living. One referrer noted “we tend to rely a lot on, you know their carers or their family in regards to provide that sort of support” (RF2). By providing practical support with daily tasks, the CTC service was able to support families who were struggling to balance caring with the demands of their own work.
There were things that I was saying would really help like could they just get mum to her covid vaccination, take her there to that appointment because I had so much time off work. (SU1)
The service was also seen as a valuable source of emotional support by families/carers.
Supporting carers I think is a really critical role I don’t know whether that’s supposed to be part of it but it definitely did make a difference for me just being able to debrief about some of the frustration, the emotional rollercoaster of the whole thing. (SU1)
Bridging the Hospital to Home Transition
Referrers felt the CTC service helped “bridge the gap” (RF1) between hospital discharge and securing ongoing home support for the client.
I’ve never had any experience with any other service that is able to sort of bridge that gap in between the person leaving hospital and before the normal carer’s package sort of kicks in. (RF2)
Referrers noted that there was often “a bit of a waiting list” (RF2) for clients to access services once discharged, causing delays between client discharge from hospital and the commencement of relevant support services. One referrer noted there was often “two to three weeks delay where they will have a gap where no one had come and reviewed them” (RF1). The CTC service bridged that gap. The practical aspect of the CTC service was perceived as unique and beneficial in ensuring clients could safely return home.
There wasn’t really any service with regards to making sure that the older person was actually safely being discharged from home, making sure that they had access to food in the fridge or making sure that they had their tablets. (RF2)
Without any service bridging the gap between discharge and home support services, referrers were inclined to keep clients in hospital for longer, until appropriate supports had been arranged, leading to “an unnecessary hospital stay in order to get the supports in place” (RF2).
Building Confidence
Referrers felt the CTC service enhanced the confidence of clients, their families, and the medical team, helping clients feel confident they could manage on their own.
Sometimes it’s just that whole confidence thing. Being in hospital, you know there’s a nurse who does everything for you and then suddenly you go home and you have to do it all by yourself […] they might not need something long term, they might just need it for a couple of days. (RF2)
The CTC service helped clients’ families feel more confident about their family member’s discharge, as well as helping referrers feel confident, they could safely discharge the patient and the patient would be supported.
I personally found it quite useful if we had clients who we were sort of on the fence about in terms of whether they could go home, we found that having that service available there to kind of link them in it gave us a bit of reassurance in sending them home and they gave the clients and their families reassurance as well. So, I do think it did help to facilitate discharges. (RF3)
Eyes in the Home
Both referrers and the CTC staff commented that the service provided a means of understanding the level of functioning clients exhibited at home, and the support clients required to safely return home. “Eyes in the home” was a phrase used by the CTC to signify the act of observing the client’s home and how they functioned within it.
Just getting them in their own environment and see, is their house cluttered? They get discharged from hospital, they get given a […] walker, but they might not have enough circulation space in their homes to actually use it, so they won’t use it and then they’ll just fall again. (SP2)
If a client was readmitted to hospital, the information gathered through having “eyes in the home” informed the medical team of how well the client functioned in their home and the supports they needed. This knowledge helped medical teams make subsequent decisions about patient discharge and provision of home support services.
When they do get readmitted, having the collateral from the [CTC] service, of how they’ve been managing at home, has been quite helpful in terms of our decisions and where we decide to go in their readmission. (RF3)


Comments (0)