
Remember me



Donor candidates were required to be healthy individuals above 18 years of age, with the majority being relatives, spouses, or close friends of the recipients [9, 10]. Before acceptance, all potential donors underwent a comprehensive preoperative evaluation, including physical examination, laboratory tests, psychological assessment, and legal screening to rule out coercion in donation [9, 10].
A computed tomography (CT) angiogram of the abdomen and pelvis was routinely performed to assess renal anatomy, vascular structures, kidney size, presence of multiple vessels, and any lesions or anomalies. Some institutions also incorporated 3D vascular reconstruction for enhanced visualization. Additionally, a Tc-99 m DTPA renal scan was utilized to evaluate glomerular filtration rates (GFR) of both kidneys, ensuring that the dominant kidney (≥ 55% function) was preserved for the donor [9,10,11].
While the left kidney was the preferred choice for procurement due to more favorable vascular anatomy, in cases where the right kidney demonstrated better structural characteristics or function, it was selected instead. All donor candidates underwent multidisciplinary board review to confirm their eligibility for surgery [9,10,11].
Surgical TechniquesRDN technique has evolved across institutions but remains consistent in its core principles. The patient is positioned in lateral decubitus, depending on the kidney selected for donation. The da Vinci Robotic Surgical System (Intuitive Surgical, Sunny Valley, CA) was used in all reported cases [9,10,11,12,13,14,15,16,17,18].
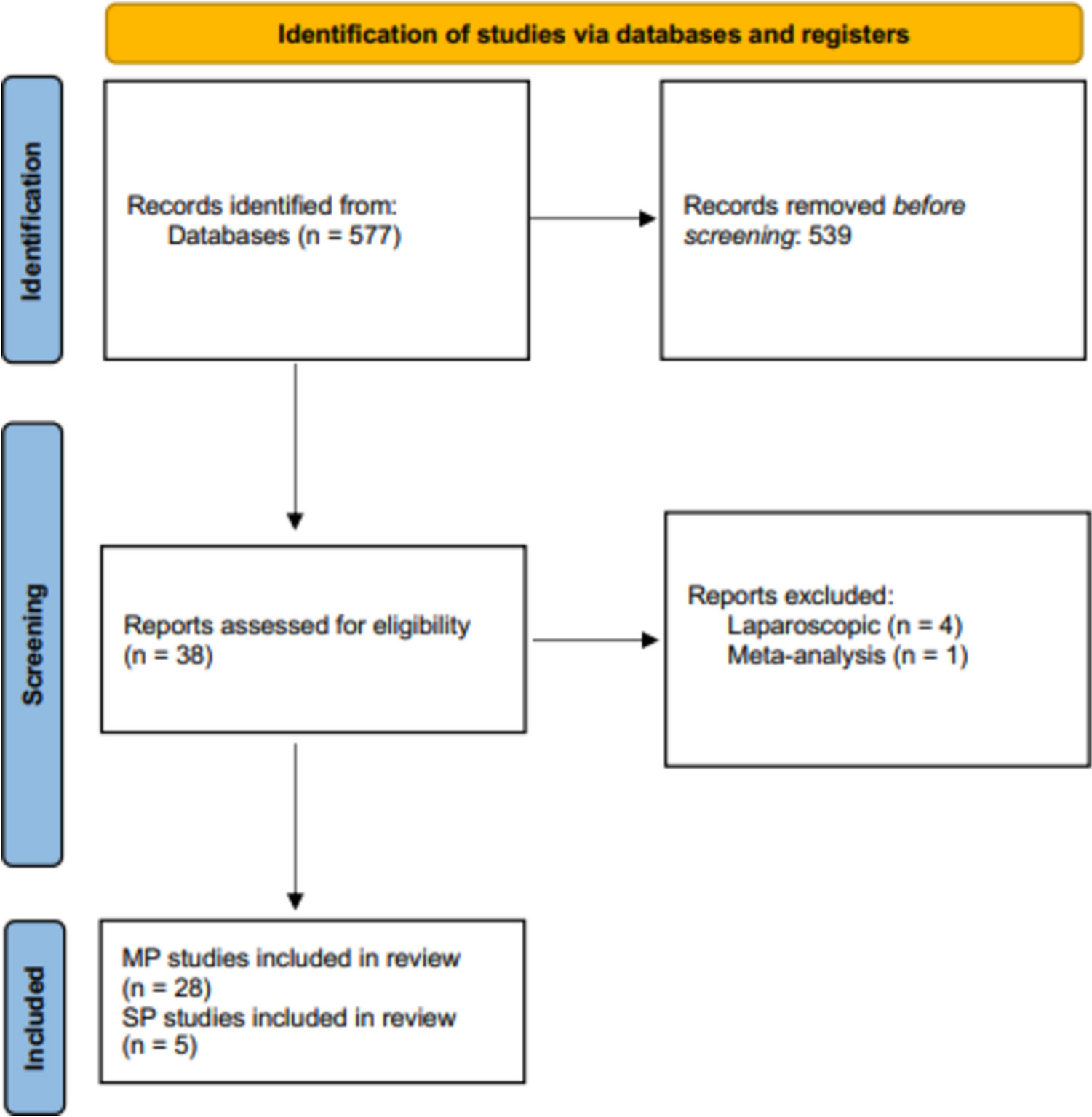
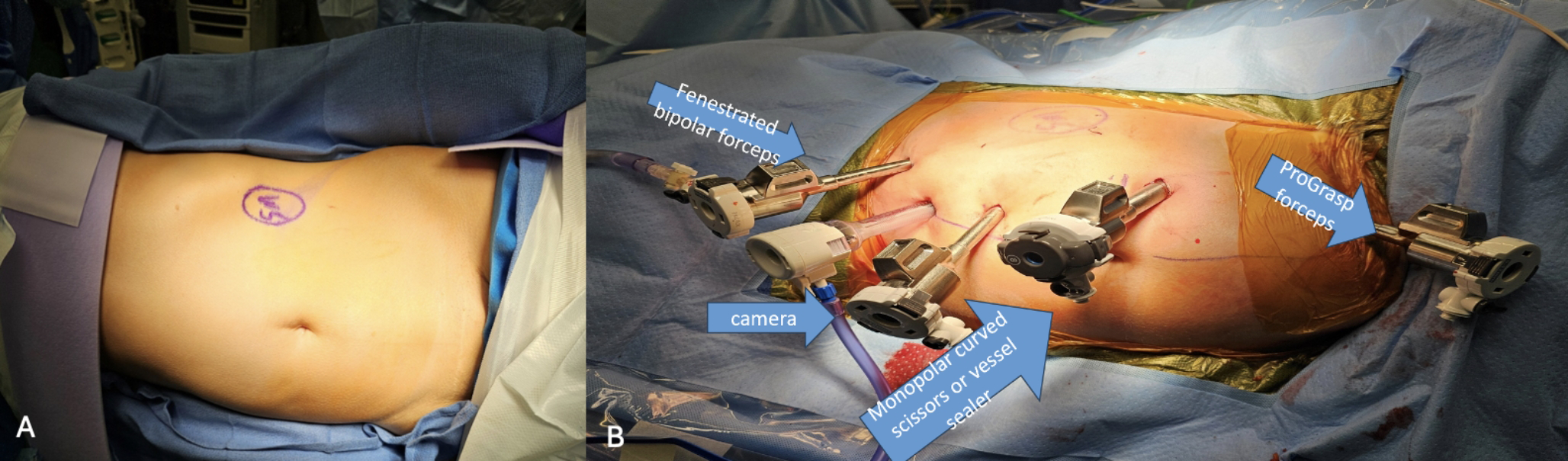
Most centers employed three to four robotic trocars: two to three 7–8 mm trocars and one 12 mm trocar for the robotic stapler. Typical port placements included subxiphoid, periumbilical paramedian, iliac fossa, and suprapubic positions. More recent studies reported using a Pfannenstiel incision for kidney graft extraction, offering better cosmetic and postoperative outcomes [9]. Some centers used GelPort-assisted extraction, while others preferred a fascial incision that was preserved until graft retrieval [11] (Fig 1).
Fig. 1
A) Patient positioning, B) Port placement
Operative OutcomesThe reviewed studies included a total of 1,846 robotic-assisted donor nephrectomy cases. Most donors were female (59%), with a mean age of 48.9 years (range 18–72 years). The left kidney was procured in 91% of cases due to its anatomical advantages.
Operative times varied between institutions, but warm ischemia time (WIT) remained consistently low, averaging 3.8 min. Estimated blood loss (EBL) was generally less than 150 mL, reflecting the minimally invasive nature of the technique. Conversion to open surgery was rare, reported in 0–3.9% of cases.
Postoperative OutcomesHospital LOS remained short, with most donors being discharged within 3 to 5 days postoperatively. Perioperative complications were minimal, with reported rates ranging from 0 to 17%, the majority classified as Clavien-Dindo Grade 1 or 2, requiring no major interventions.
Recipient OutcomesAmong kidney transplant recipients, delayed graft function (DGF) was observed in 1.7–11.5% of cases. At last follow-up, mean estimated glomerular filtration rate (eGFR) ranged from 57 to 64 mL/min/1.73 m², and serum creatinine levels were stable between 1.1 and 1.37 mg/dL. Vascular and ureteral complications were rare but reported in a small subset of cases (Tables 1, 2).
Table 1 Study characteristics and operative dataTable 2 Donor postoperative and recipient outcomes
Comments (0)