Limited molecular profiling in SEA and the need for expansion
Molecular profiling in SEA remains significantly underutilised in UM, as prognostic testing in Asia relies on the IHC assessment of BAP1 loss [3, 43]. While numerous studies have confirmed the sensitivity and specificity of this IHC technique [44,45,46], its use is often hindered by technical issues that can lead to inaccurate assessments [45]. In our study, BAP1 IHC was used to assess its association with survival outcomes (Fig. 2), reflecting the reliance on this method in current clinical practice. However, it is essential to acknowledge that while BAP1 IHC provides critical prognostic information, it may not fully account for other genetic and molecular factors influencing UM prognosis. This underscores the urgent need to expand molecular profiling in SEA to include advanced techniques, such as next-generation sequencing or whole-genome copy number analyses, which could complement IHC and refine prognostic accuracy. Broadening the scope of molecular testing would also help address regional disparities in UM research and improve personalised treatment strategies for patients in SEA.
Monosomy 3 and chromosome 8q in the asian context
While it is well-established that monosomy 3 and gains in chromosome 8q correlate with poor prognosis [9, 13, 29, 30, 47, 48], our study found that only monosomy 3 was significantly associated (P = 0.0438) with reduced PFS. The loss of BAP1 nuclear expression was also linked to shorter PFS, which matched the BAP1 gene expression in the TCGA-UM cohort. We also observed that the frequency of monosomy 3 was much lower in our Asian patients compared to the TCGA-UM cohort and other studies from the West [35, 39, 40]. Although associated with shorter PFS, the lower frequency of monosomy 3 in our cohort raises the possibility it does not play as great a role in UM metastasis and that other factors could be more critical for the disease.
Contrary to previous reports that associate 8q gains with poorer outcomes [14, 29, 30], our study found that only gains in chromosome 8p, not 8q, were linked to shorter PFS in our Asian cohort. While recent publications suggest no significant difference in survival based solely on iris colour, other studies indicate that aberrations in chromosomes 3 and 8q tend to have a more pronounced impact on patients with light-coloured irides compared to those with brown irides [48, 49]. This disparity may be attributed to differences in pigmentation and tumour biology. In our cohort, the predominance of brown irides and Fitzpatrick Skin scale III–V may partially explain why chr 8q gains were not associated with poorer outcomes. This observation aligns with the hypothesis that chromosomal aberrations such as 8q gains may be less prominent in populations with darker irides. By highlighting these differences, our findings contribute to the growing evidence that genetic and phenotypic factors, including iris colour and Fitzpatrick skin tone, may modulate the prognostic significance of specific chromosomal alterations in UM. In the TCGA cohort, patients with Fitzpatrick Skin Scale I and lighter irides were more likely to have higher grade UM compared to Fitzpatrick Skin Scale II, and III–V patients [50]. A recent study by Agrawal et al. [51] found that patients with Fitzpatrick Skin Scale III-V and brown irides had UM of larger thickness and basal diameter that corroborates with our findings. Of note, our four patients with metastasis were of the lower Fitzpatrick Skin Scale III in comparison with the rest of our cohort that ranged III–V, suggesting that skin tone is a more sensitive prognostic factor in Asians rather than iris colour, which has no grading system like the Fitzpatrick Skin Scale.
The significance of chromosome 1q gains in Asian UM tumor progression
In our study, chromosome 1q gains, as well as chromosome 8p losses and 8p gains, were associated with shorter PFS in the SEA UM cohort. The observed frequency of 1q gains in our cohort (20%) was notably higher than that in the TCGA-UM cohort (6%) and aligns with previously reported frequencies of approximately 24% in other studies [29]. While chromosome 1q gains have been associated with poorer prognosis [29], their specific role in UM progression remains poorly understood, and research explicitly examining their impact in UM is limited. A recent study by Shain et al. on metastatic UM demonstrated that chromosome 1q gains were significantly enriched in metastatic tumours, often emerging later in disease progression following the loss of BAP1 [52]. This suggests that 1q gains represent a late event contributing to UM metastasis. In our SEA cohort, where delayed diagnosis remains a challenge, patients often present with more advanced disease, and this may contribute to the observed higher frequency of chromosome 1q gains since it occurs as a late event in the mutational timeline. These findings suggest the importance of early detection and treatment in Asian UM to mitigate the development of such late-event high-risk genetic alterations. Interestingly, in the TCGA-UM cohort, the trend of shorter PFS associated with chromosome 1q gains observed in our SEA cohort was not evident, further underscoring potential differences in genetic and clinical behaviour between Asian and Western UM populations (Fig. 2c).
The formation of isochromosomes, particularly involving chromosome 1q, may provide additional insights into the mechanisms underlying 1q gains in UM. Previous research [53] suggests that genomic instability caused by the loss of chromosome 3 can lead to the formation of isochromosomes, including those involving chromosome arms such as 1q, 6p, and 8q. This mechanism could explain the additional copies of 1q observed in our cohort, potentially in cases with concurrent monosomy 3. However, compared to the Western populations, the relatively low frequency of monosomy 3 in our SEA cohort suggests that 1q gains occur independently of chromosome 3 loss in some patients. This highlights the need for further research to explore the formation of isochromosome 1q in relation to monosomy 3 and its role in UM progression, especially in non-Western populations.
The distinct genetic landscape observed in our SEA cohort, where chromosome 1q gains were more frequent compared to the TCGA-UM cohort and were associated with shorter PFS together with the lower monosomy 3 frequency reflect differences in the underlying genetic mechanisms of metastasis between SEA and Western populations. These findings emphasize the need for the expanded study of genetic alterations in individuals with different iris colours and skin tones to further elucidate and understand such potential differences.
Chromosome 6p loss and metastatic potential
In our study, chromosome 6p loss was the most frequently observed chromosomal aberration among patients with metastasis, present in about 50% of these cases. This finding aligns with other studies linking 6p loss to increased metastatic risk in UM [14]. In the patient with the shortest RFS and liver metastasis, chromosome 6p losses were present with other high-risk aberrations such as losses in chromosome 1q and gains in chromosome 8q, but notably without monosomy 3. This suggests that genetic aberrations without monosomy 3 such as chromosome 6p loss, together with other high-risk aberrations can be as aggressive as tumours with monosomy 3 that are known to have earlier metastasis. Whilst this raises a possibility that in Asian UM, the higher frequency of 6p losses and other non-monosomy 3 high-risk mutations can drive metastatic risk, we are cautious of drawing further conclusions due to the low statistical power of our study. Further studies with larger cohorts are needed to confirm our observation of the metastatic potential of 6p loss with other non-monosomy 3 chromosomal aberrations in Asian tumours.
Chromosome 9q gains: a potential protective biomarker
Gains in chromosome 6p are the only aberration associated with a favourable outcome [48]. In our study, chromosome 6p gains did not demonstrate a statistically significant “protective effect” against metastasis but showed a trend toward a longer PFS. However, the study did not have sufficient power to either confirm or exclude the possibility of this protective effect, given the small sample size. Interestingly, chromosome 9q gains were significantly associated (P = 0.0057) with longer PFS in our cohort, suggesting a protective role. Chromosome 9q gains have not been widely reported as prognostic in UM. However, a small case series of Vietnamese UM patients with 9q gains and no metastasis was observed during a 3-year follow-up which appears to support our observation [54]. The clinical significance of this needs to be further evaluated as this was not observed in the TCGA-UM cohort.
Mutation burden differs with age—a possible bimodal age of presentation
Our mean age of diagnosis was 57 ± 17 years, reflecting this trend of a younger age of presentation in Asian populations. This distribution aligns with findings from Manchegowda et al. who reported a generally younger mean age of presentation in Asian UM patients compared to Western populations, ranging from 42.9 to 63.5 years [3].
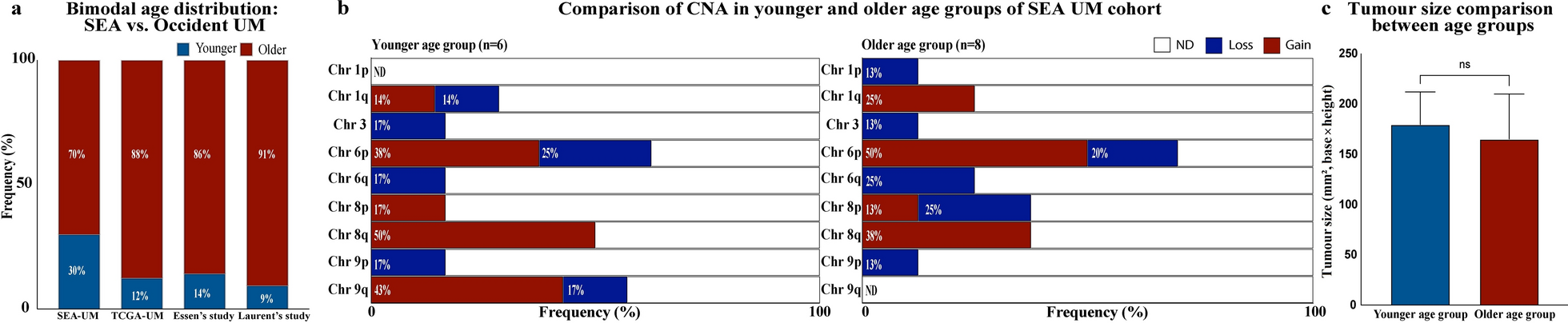
However, when using a cut-off age of ≥ 45 years, we observed a bimodal age distribution in our SEA cohort, with a younger subgroup presenting at a median age of 35 years (range: 30–45 years) and an older subgroup at a median age of 66 years (range: 52–77 years), that is similar to the median age reported in the West [1].
To determine if this bimodal age distribution was due to tumour volume, we compared the tumour volume between these two age groups (Fig. 1c) and found no statistically significant difference, indicating that the tumor size at presentation was similar regardless of age. In the same vein, when comparing the survival outcomes in these age subsets, there was no statistically significant difference between the younger and older age groups. However, the overall survival rate was slightly higher in the younger subgroup (83%) compared to the older group (70%). Among patients < 45 years old, only one patient experienced UM-related mortality due to kidney metastasis (Table 3), indicating a relatively favourable survival profile in the younger group.
An age-related difference in genetic landscape comprising a higher frequency of chromosome 1q gains, 8p losses, and a smaller increase in chromosome 6q and 1p losses was noted in the older age subset compared to the younger subset of patients (Fig. 1b), which may further support a possible bimodal age of presentation.
Whilst this bimodal age distribution may reflect inherent detection bias or systematic differences in tumour presentation due to our small sample size, it highlights the possibility of differences in demographic and genetic characteristics that may be unique to Asian populations. Again, future studies with larger cohorts are necessary to investigate any potential associations between age at diagnosis, genetic profiles, and tumour characteristics in UM before further definitive conclusions can be drawn.
Tumour size and histology
Our study's tumour sizes and histological findings are similar to other reports studying Asian populations, where spindle cell histology is more commonly observed [3]. However, according to the TNM classification, 65% of the tumours in our cohort were classified as large or very large, and almost half of our tumours (9/20, 45%) were stage III tumours (Table 2, Supplementary Fig. 2), reflecting a high proportion of advanced tumours at diagnosis. This observation underscores the challenges of delayed diagnosis in Southeast Asia, where limited awareness of UM often causes patients to assume that the vision loss is attributed to more common conditions such as cataracts which in turn leads them to seek treatment when the loss in more severe. Such delays likely contribute to our study's large tumour sizes and advanced stages. Interestingly, we found no significant difference in tumour size between younger and older patients, suggesting that delayed diagnosis and its associated challenges are not confined to specific age groups but are a widespread issue across the SEA population. These findings highlight the need for increased awareness and earlier detection strategies to improve regional UM outcomes.
Survival and metastatic rates
The 5-year OS in our cohort was 75%, within the wide range reported in Asia (53%–92%), and is only slightly higher than the 70% OS observed in the TCGA-UM cohort [35] and the 62%–70% reported in the West [3, 55]. The 5-year RFS/PFS rate in our cohort was 70%, similar to the PFS rate of 69% reported in the West [37] and 64% observed in the TCGA-UM cohort [35]. Similarly, the metastatic rate of 20% in our patients was only slightly lower than reported metastatic rates of up to 26% from USA cohorts [20, 41, 56]. In a study of a large series with more than 8000 patients by Shield et al., they found the 10-year metastatic rate for choroidal melanomas to be 25% [57]. Our observed rate of metastasis in our small cohort was also observed in a large Chinese series of 171 patients with a metastatic rate of 21% [5]. This indicates that metastatic rates are similar in the Asian and Western populations despite UM’s rarity in this region and raises a possibility that in Asia, other genetic mutations may play a more significant role in metastatic risk.
In Shield and colleagues’ report [57], they also highlighted the importance of tumour size in relation to metastatic risk. Although our SEA cohort had a high number of large and very large tumours, our data indicated no significant association between tumour size or histological subtype and metastasis, and this appears to deviate from their finding and commonly accepted knowledge. Additionally, in our small cohort, spindle cell melanomas were observed to metastasize more frequently than epithelioid melanomas. This unexpected finding may be due to our limited sample size, which reduces the statistical power to detect definitive associations and could introduce variability. These observations underscore the importance of future collaborative studies with an Asian Uveal Melanoma Registry like the TCGA cohort to allow us to study larger cohorts to validate or refute these findings and explore potential biological mechanisms that may underlie these differences.
Limitations and future directions
Limitations of using the TCGA-UM dataset: The TCGA-UM is a series of publicly available tumours obtained from six institutions (four centers from the USA, one UK and one French Center, with more than 70% of the cases from UK and France) and unlike our series, were selected cases over 2003–2017 [35], whereas our SEA cohort is a single center consecutive case series analysis over 2004–2018.
In comparison to our cohort, none of the TCGA-UM tumours (n = 80) was classified as T1 tumours (compared 10% of our SEA cohort), and although the percentage of T2a and 2b tumours were similar 17.5% (17/80) in the TCGA-UM cohort vs. 20% (5/20) SEA cohort, most of the TCGA-UM tumours (66/80, 83%) were pT3 and larger [35], whereas only 65% (13/20) of tumours in our SEA cohort fell into this category (Supplementary Fig. 2). The higher proportion of larger tumours and the presence of metastasis at diagnosis in four patients from the TCGA-UM cohort, compared to none in our cohort, also indicate that the TCGA-UM cohort included more advanced and aggressive UM tumours. This may explain why the number of cases with metastasis during follow-up was higher in the TCGA-UM cohort (33 cases, 41%), which is double the rate observed in our SEA cohort (four cases, 20%).
Whilst the comparison with the TCGA-UM cohort provides meaningful context, there are differences in the TCGA cohort and our SEA cohort that limit direct generalizability, underscoring the need for multi-regional comparative studies across geographic regions to reflect real-world data.
Another limitation of our study is the small sample size which reflects the rarity of UM in Southeast Asia but also emphasizes the need for similar studies from other centers in this region for real-world data analysis. Despite the limited number of cases, our findings highlight key differences in genetic alterations, offering preliminary trends that may encourage similar future research. In previous studies from Asia, the relatively shorter follow-up duration may underestimate late-onset metastasis, and the absence of advanced molecular profiling techniques, such as next-generation sequencing, limits the depth of our genetic analysis. However, the use of the OncoScan™ CNV Array permits us to identify critical chromosomal alterations that influence UM progression.
Despite these limitations, this study has several strengths. It focused on a rare, understudied Asian population and provided insights into critical prognostic markers like monosomy 3 and polysomy 8 while highlighting the potential role of other chromosomal aberrations, such as chromosome 1q gains and 6q losses, in association with metastatic disease. It also reveals the need for better awareness and earlier diagnosis of UM in Southeast Asia, offering valuable clinical relevance by encouraging the use of molecular profiling in the region.
The lower incidence of monosomy 3 in our local population raises concerns about whether relying solely on BAP1 loss, assessed through gene expression or immunostaining, is sufficient for metastasis surveillance and risk stratification in Asian patients. The association of other cytogenetic abnormalities, such as chromosome 1q gains and both chromosome 8p losses and gains, with shorter PFS suggests that these mutations may play a more significant role in the metastatic process in Asians. Investigating the impact of these chromosomal aberrations in other Asian cohorts and conducting gene expression profiling will be crucial for further clarifying their roles and uncovering downstream mechanistic insights and represent our directions for future research. In addition, the role of PRAME IHC or mRNA expression may be a useful alternative in SEA and represents our future area of research. This, together with GEP analysis, may be useful for UM prognostication in SEA.





Comments (0)