
Remember me









The fact that psychological problems—think of anxiety, lack of attention or a persistently low mood—are often viewed as brain problems today can be seen in the increasing number of prescriptions for various psychotropic drugs. One example of this are the stimulants amphetamine and methylphenidate, which are prescribed as drugs called Adderall and Ritalin, among other brand names. This often happens after a diagnosis of attention deficit/hyperactivity disorder (ADHD).
In fact, many decades ago, such stimulants were used on a daily basis by many to reduce fatigue or improve mood (Rasmussen, 2008). They used to be available without a prescription, but since the “War on Drugs” they have been considered dangerous narcotics. Amphetamine was and is popular as a street drug, then named “speed,” and for military purposes (Snelders & Pieters, 2011). And although the World Health Organization (WHO) already warned in the 1990s about the sharp increase in the administration of these drugs, particularly to children, prescriptions have multiplied since then (Schleim, 2023). Despite this decades-long increase, just as I write these words, another article appeared in the New York Times and claimed that ADHD in adults is still too often overlooked.Footnote 2
This is just one example of what it can mean to understand mental health problems as brain problems: Then a “solution” with pharmacological means seems obvious. The theoretical foundations, individual and social consequences of this practice have already been discussed elsewhere (Davis, 2020; Szasz, 1974; Valenstein, 1998). For us, the precursors of the “Decade of the Brain” are relevant at this point.
1.1.1 The Brain as an Organ of the PsycheIt is often forgotten that mental disorders were already regarded as physical illnesses in ancient times. A clear testimony to this is a visit by the famous physician Hippocrates (c. 460–c. 370 BC) to the materialist natural philosopher Democritus (c. 460–c. 370 BC). The latter suffered, as we would probably say today, from depression. When the doctor came to see him, he found dissected animals at his patient's home. The philosopher explained this as follows:
How could I otherwise write on the nature of madness, its causes and the mode of alleviating it? The animals which thou seest here opened – I opened them not because of hate of the work of the divinity, but because I am searching for the seat and the nature of bile; for thou knowest it is usually, when it is excessive, the cause of madness. (quoted from Zilboorg & Henry, 1969, p. 45)
The idea that diseases are caused by an imbalance of humors in the body has influenced medicine for thousands of years, in both Western and Eastern cultures, in the north and south of the globe (Hall, 1971). The name “melancholia” (Gr. mélas = black and cholé = bile) bore witness to this until our recent past (Fig. 1.1).
Fig. 1.1
Edvard Munch (1863–1944) who himself had severe psychological problems painted “Melancholy” in 1893. Today he might have called it “Depression.” The example illustrates the historicity of the way we talk about mental states (License: public domain)
On the way to what we now call “major depressive disorder,” there was still the intermediate step of “melancholic depression” in the twentieth century (Shorter, 2015). Long before the discovery of neurotransmitters, it was assumed that depressed mood, for example, was caused by an excess of black bile. However, anatomical research in modern times revealed that this substance, which was thought to be found in the spleen, does not actually exist. Its alleged role was given to the neurotransmitter serotonin in the twentieth century, but then as an assumed deficiency instead of an excess; however, the serotonin hypothesis of depression is still controversial today (Cowen & Browning, 2015; Moncrieff et al., 2023; Valenstein, 1998). And who would have expected that the recent ICD-11 of the WHO reintroduces a “melancholic depression,” such that the ancient “black bile disease” still casts its shadows into our times?
So if biological psychiatry presently assumes that mental disorders are physical disease entities, as in other parts of medicine, then this thinking is not new. Over time, however, the brain gained in importance as the central organ of psychiatry. Wilhelm Griesinger (1817–1868) is sometimes regarded as the “father of neuropsychiatry” because in the mid-nineteenth century he clearly described mental disorders as brain diseases (Schleim, 2022). However, such efforts can be traced back to the seventeenth century (Berrios & Marková, 2002) and even antiquity (van der Eijk, 2005).
Speaking of melancholy, the English physician and pharmacist John Haslam (1764–1844) is another example worth mentioning. In 1809, he published the second edition of his Observations on Madness and Melancholy which described 37 case studies with brain examinations after the death of the patients. From these observations he concluded:
From the preceding dissections of insane persons, it may be inferred, that madness has always been connected with disease of the brain and of its membranes. […] It may be a matter, affording much diversity of opinion, whether these morbid appearances of the brain be the cause or the effect of madness: it may be observed that they have been found in all states of the disease. (Haslam, 1809, pp. 238–239)
This coincided with the emergence of phrenology, which linked psychological faculties to areas of the brain and externally recognizable characteristics of the head shape. Of course, the proponents of this doctrine also claimed that mental disorders were based on organic brain disorders; we will return to this briefly in Chapter 3. However, Haslam was not a phrenologist and cited the Irish philosopher John Toland (1670–1722) in support of his theory, who in his Pantheisticon of 1720 described all thinking as a function of the brain.Footnote 3
In addition to discussing the question of whether the characteristics he found in the brain really are the causes of mental disorders, Haslam also made some other extraordinarily modern and topical observations. I will therefore briefly discuss two of them: For example, he argued that mania and melancholia should not be understood as separate disorders because, firstly, he had not been able to identify any brain differences between them and, secondly, the treatment was the same. He refuted the alternative hypothesis that these are not physical but rather mental diseases by pointing out that material medical procedures—but not logical-rational methods—worked.
We do not know exactly what John Haslam thought he saw in the brains of these patients around 1800; he described tissues as abnormally soft or firm (for illustrative purposes: Fig. 1.2). But we do not need to establish a history of psychiatry or medical psychology here, as the discipline was once called (Horwitz, 2020; Zilboorg & Henry, 1969). For our purposes, it is relevant that the search for “the psyche” in the brain is still ongoing today. We should keep these historical examples in mind when we now turn our attention to the new waves of neuro- or biological psychiatry in the twentieth century. Particularly when we look at the allegedly revolutionary idea of “broken brains” in the 1980s, we will understand the historical background of this thinking.
Fig. 1.2
(Source Amsterdam Museum. License: public domain)
Haslam's sections may have resembled “The Anatomy Lesson of Dr. Deijman” (1656), which the Dutch master painter Rembrandt van Rijn (1606/1607–1669) captured on this canvas. However, only this fragment survived a fire in 1723. On the dissection table lies the body of Joris Fontein, who died in his early 20s: he was caught in the act of burglary, confessed (under torture) to numerous other crimes and was sentenced to death by hanging. After his execution, his body was given to the Amsterdam Surgeons’ Guild. We do not know whether the dissecting doctor searched the dead man's brain for the cause of the crime; if so, it would be an early example of neurolaw. However, surgeons recently determined from a replication of the dissection that the pose depicted presupposes a broken neck, as can occur during hanging (IJpma et al., 2013)
1.1.2 “Broken Brains”Psychiatry had many faces in the twentieth century. Under the influence of Sigmund Freud (1856–1939), the psychodynamic approach led the way for several decades. According to this view, mental disorders often arise from unconscious conflicts in the “psyche” that are frequently associated with early childhood experiences. The disorders are then to be treated primarily with talk therapy, for example with psychoanalysis, to make the unconscious dynamics conscious and thus resolve the conflicts. The American diagnostic manuals DSM-I from 1952 and DSM-II from 1968 were strongly influenced by this kind of thinking (Mayes & Horwitz, 2005).
In the 1930s–1970s, however, there were major breakthroughs in the field of biological or neuropsychiatry: think of the use of brain surgery, brain stimulation and pharmacology, for example lithium and chlorpromazine. At the time, these were even applied to criminal law problems, as an article in Popular Science Monthly shows (Fig. 1.3).
Fig. 1.3
(Source: created with Adobe Firefly)
“Have You a Wrong Way Brain?” asked the headline of an article in the July 1939 issue of Popular Science Monthly. Inspired by brain surgery, the author speculated that criminal behavior occurs when the less dominant hemisphere of the brain takes control and “Dr. Jekyll becomes Mr. Hyde” or a loving father becomes a villain. He also wrote that up to 85 percent of prisoners suffer from mental disorders and procedures such as lobotomy or insulin shock therapy—both no longer used today—could solve the problems. The concluding sentence was: “By cutting the roots of crime in the minds of malefactors, they may some day play a major role in reducing our $15,000,000,000-a-year crime bill and in turning outlaws into good citizens”
However, the high expectations turned out to be exaggerated time and again and—sometimes very severe—side effects eventually received more attention (Delgado, 1971; Schleim, 2021; Valenstein, 1973, 1998; Williams et al., 2008). The lack of more objective criteria for diagnosis, such as blood, genetic or brain tests, led to confusion. For example, schizophrenia was diagnosed more frequently in New York, but depression more frequently in London. Finally, studies with standardized material showed that psychiatrists in the USA and Great Britain had different ideas about these disorders (Kendell et al., 1971; Schleim, 2023).
With advances in genetics, imaging techniques and the information sciences, which we now summarize as “neuroscience,” the dream of a modern scientific psychiatry seemed within reach. For the DSM-III of 1980, a group of psychiatrists who found the old psychodynamic categories too speculative and who wanted to adapt the discipline to scientific advances finally prevailed (Mayes & Horwitz, 2005; Wilson, 1993). This thinking still characterizes the DSM today. But this advance also implied the removal of the etiology, the theory of causes, from the diagnostic manual and working groups at the conference table agreed on the now well-known checklists for several hundred mental disorders.
Until the much-delayed DSM-5 was published in 2013, one of the main objectives was to provide the neurobiological etiology that was missing from the new approach (Hyman, 2007). At the turn of the millennium, much was expected from genetics and brain imaging research in particular. For example, studies such as the one by Ingvar and Franzén had already reported differences in the blood flow of the frontal brain of people diagnosed with schizophrenia in the 1970s (Ingvar & Franzén, 1974). Prior to this, over 100 years of anatomical brain examinations of deceased patients with such severe disorders had not provided any clarity. Proponents of this approach, such as the German-Austrian neuroanatomist Theodor Meynert (1833–1892), who localized mental disorders only in the frontal brain (Meynert, 1884), were even accused of practicing “brain mythology” by psychiatrists focusing on actual patients in the clinics (Marx, 1970).
In the twentieth century, interest in this approach to psychiatry continued in waves (Fig. 1.4). Thanks to new scientific procedures and the new categories of the DSM-III, the 1970s and 1980s were characterized by a spirit of optimism. We already saw this in Roger Sperry's far-reaching statement at the beginning of this chapter (Sperry, 1981) and it is also very well illustrated in Nancy Coover Andreasen's much-cited book The Broken Brain: The Biological Revolution in Psychiatry from 1984. The American psychiatrist became one of the leading experts in the field of schizophrenia, helping to shape both the DSM-III of 1980 and the DSM-IV of 1994, and for 13 years was editor-in-chief of the American Journal of Psychiatry. In her book, she announced a revolution in research, diagnosis and therapy through the biological model. In her words:
In more recent times the biological model has been shaped by the growth of the discipline ‘neuroscience’ or the neurosciences. […] Much of the time these abnormalities [in behavior, emotions, and thinking, St. S.] cannot be traced to a distinct area of damage in the brain, although the biological model assumes that as our knowledge progresses, some type of malfunction in the brain will be found. The current biological revolution in psychiatry places great emphasis on the search for the physical causes of mental illness. (Andreasen, 1984, pp. 27–28)
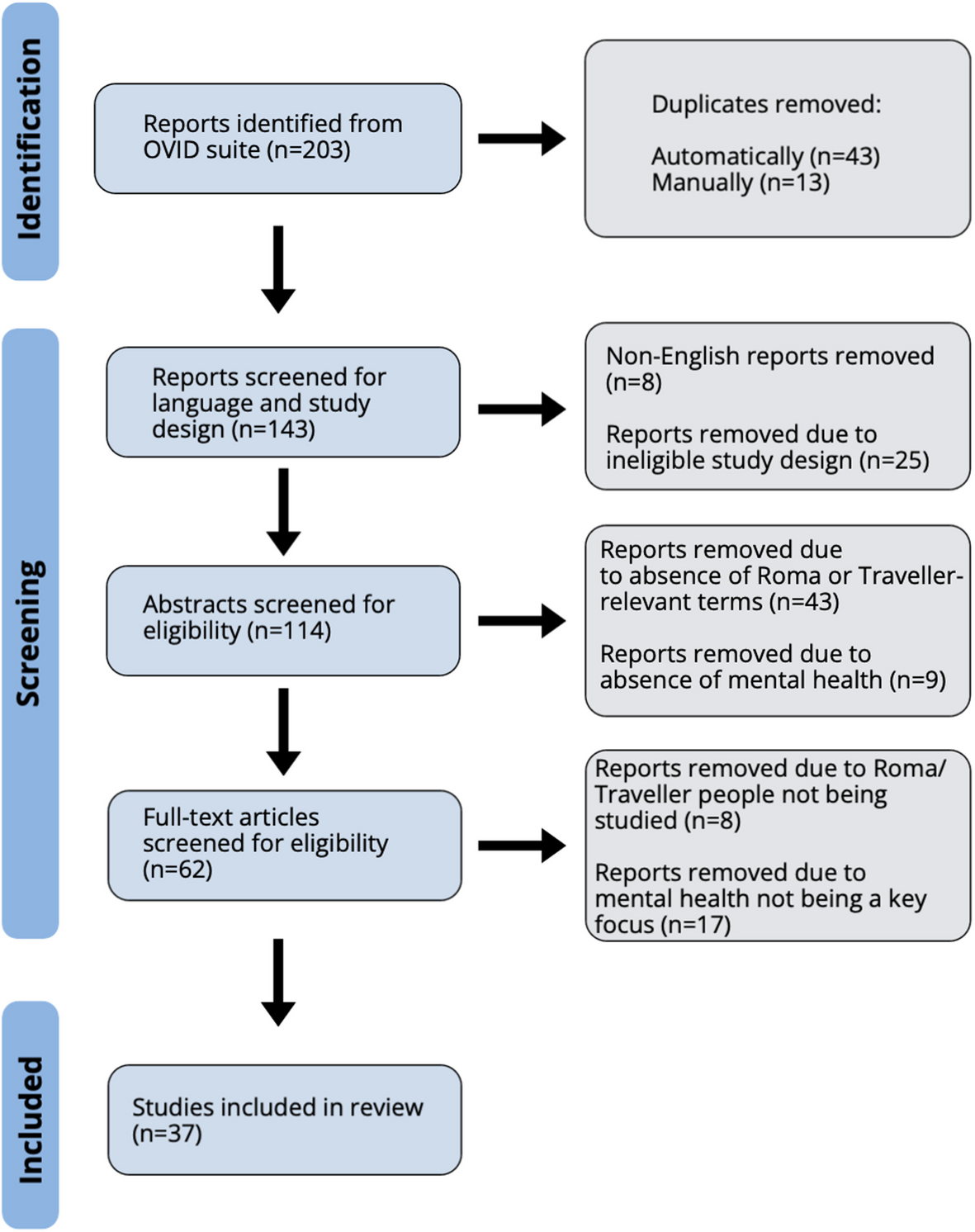
Fig. 1.4
(Source Google Ngram)
This Google Ngram shows the relative frequency of the terms “neuropsychiatry,” “biological psychiatry” and “clinical neuroscience” in English-language books. The large spike in the 1940s and 1950s coincides with the spread of psychosurgery and new psychotropic drugs. Later, other terms also appear more frequently. However, it should be borne in mind that in the course of the twentieth century, publications in books became less important in research and were increasingly replaced by articles in specialist journals (scale: 10−8 percent)
The goal was therefore clear: to find the dysfunctions in the nervous system at a cellular or molecular level that cause mental health problems. In addition to electroencephalography (EEG), which had already been developed in the 1930s, new imaging techniques such as computer tomography (CT), positron emission tomography (PET) and functional magnetic resonance imaging (fMRI)—which was only developed a few years after Andreasen's book—were to provide deeper insights into the living human brain than ever before. With the help of genetic, pharmacological and electrical tests in animals and humans, the underlying mechanisms should be identified. Andreasen explains this with a case study, which I would like to reflect upon below. But first, some basic knowledge about how imaging techniques work.
Understanding NeuroimagingImaging techniques have become an integral part of medicine, for example in the search for tumors or the examination of the fetus during pregnancy. But their importance for research has also steadily increased. Today, brain scans are one of the most important measurement methods not only in neuroscience, but also in psychology and psychiatry (Friston, 2009). The distinction between structural and functional methods is important.
Structural procedures make different types of tissue or bone visible. The best known is probably still X-ray radiation, which is absorbed to different degrees by different types of tissue and thus leads to visible differences on the images. Certain—often radioactive—tracer substances, which are administered intravenously, can be used to highlight certain types of tissue, such as tumors.
In the neurosciences, functional methods are used to examine brain function instead. In the past, tracer substances were also used for this purpose, for example to visualize the consumption of the energy supplier glucose or the presence of certain synapses responding to neurotransmitters. The great advantage of functional magnetic resonance imaging (fMRI) is that it does not require tracer substances. The physiological basis for this was discovered around 1990 by the Japanese biophysicist Seiji Ogawa and his colleagues. This is based on the fact that blood has different magnetic properties depending on its oxygen saturation, which can be measured in strong magnetic fields; and the oxygen saturation is in turn associated with neuronal activity (Logothetis, 2008). However, this correlation is not perfect and oxygen saturation is only an indirect but often useful indicator of neuronal activity.
For the purposes of this book, two observations are important: First, the known brain images reflect reactions in experimental situations that can only be interpreted by comparing different conditions—often a target and control condition. Second, the colors projected onto an anatomical brain image are not a direct visualization of brain activity, but of the results of statistical tests (Dumit, 2004; Schleim & Roiser, 2009).
This means that the results of fMRI studies are dependent on the characteristics of the experiment and the evaluation by the researchers. They are therefore by no means as direct or objective representations of experience and thought as is often portrayed (Racine et al., 2010). In fact, it has now been shown that different neuroscientists can draw different conclusions from the same brain data (Botvinik-Nezer et al., 2020).
1.1.3 People in ContextsAt the beginning of her book about Broken Brains and the biological revolution in psychiatry, Andreasen referred to the problematic past and present of her discipline. In the past, people with mental health problems were persecuted as being possessed by the devil or evil spirits and, in extreme cases, even killed. The psychiatrist did not mention that they were sometimes regarded as saints. She then described the case of the American sailor William (actually James) Norris, who was brought to London's Bethlem Royal Hospital as a “lunatic” in 1800. Due to violent outbursts, he was eventually put in chains and kept in this state of severely restricted freedom of movement for around ten years.
During a parliamentary inquiry into the hospital, the appalling conditions came to light and were disseminated to the public as horror stories. A parliamentary commission set up in 1815 then led to an improvement in the conditions in British hospitals and “lunatic asylums.” Although Norris was freed from his chains, he died of tuberculosis shortly afterward—probably also due to his poor physical condition as a result of his long imprisonment.
The case was so important to Andreasen that she placed a drawing of the chained patient at the beginning of her book. According to historical reports, however, Norris was also considered manipulative and dangerous, almost killing his guard and biting off another patient's finger (Andrews et al., 1997). To alleviate his fate, he was given a cat, newspapers and books. Andreasen did not mention any of these circumstances. She also seems to have been unaware that the doctor blamed for the scandal was none other than John Haslam, the “brain doctor” we met above, thus a medical professional who wanted to advance psychiatry in the same way she did. Unfortunately, violent patients still pose practical and legal challenges for psychiatric institutions today.
Why such cases are important for our book becomes particularly clear from the portrayal of “Bill,” to whom Andreasen devoted almost eight whole pages: This psychiatric patient had studied medicine at Harvard with outstanding achievements. Toward the end of his studies, his father died. Bill's subsequent depression was treated with medication and slowly improved. However, due to his psychological problems, the examination board initially denied him his degree and required him to study for a year longer. He kept his feelings of humiliation and despair to himself.
Despite his exceptional academic achievements, he then had difficulty finding the necessary internships and a position as a junior doctor. The stigma of “psychiatric illness” clung to him. He eventually married a former fellow student, had two daughters with her and set up his own practice. He had another depressive episode treated by a psychiatrist in a community 50 miles away, as he was aware of the stigma of this diagnosis. The new drug therapy helped him.
When Bill was 35 years old, his wife was diagnosed with incurable liver cancer. She died within a year. During the last two months of her life, Bill was overcome by uncontrollable crying fits at work. Eventually, he himself was admitted to a psychiatric hospital. His terminally ill wife resented this, and his acquaintances also had little understanding for it: “Some people in the community had trouble understanding why he could not maintain better control of himself. They thought him weak and lacking in self-discipline” (Andreasen, 1984, p. 4).
After the funeral, Bill threw himself into work. He found a housekeeper to look after his daughters, who were two and four years old when his wife died. After a year, he looked for a new partner and eventually married Joann, ten years his junior. While he longed for a domestic life, she preferred to go out a lot and eventually had an open relationship. Bill could not stand her affairs with other men in the long term. When he asked her to be monogamous, she divorced him. This was the third time Bill had lost an important person: his father and his first wife through death, his second wife through divorce.
The fact that Joann stayed in the area and that he kept seeing her with new partners bothered him. After one such encounter, he got drunk and drove to her apartment in the evening. When he harassed her, Joann called the police. The local media reported on Bill's problem behavior. When he was again receiving medical treatment for depressive symptoms and could no longer make it to work every day, the public scandal was the last straw. According to Andreasen, he had no support:
After his arrest and its bad publicity, he went to pieces. Other physicians in the community knew that he had been having problems, but no one made any attempt to offer help or sympathy. Some thought he simply needed to be tougher, while others thought he was behaving irresponsibly. Having put most of his energy into his work and his family, Bill had few close friends. The two or three whom he did have held back from approaching him because of uncertainty or embarrassment. (ibid., p. 6)
In the end, he was no longer able to work and was admitted to hospital. This time, no medication helped, so they tried electroconvulsive therapy (also known as electroshock therapy). Thanks to this, he felt better again and was able to leave the clinic after six weeks—only to find that his license to practice medicine had been temporarily revoked due to his stay in the clinic. Not only did he lose his daily job as a doctor and source of income, but he was once again the subject of the press, this time even on television. His daughters, who were now at school, were also drawn into the scandal.
Bill finally took his own life at the age of 45 so that, Andreasen wrote, he could at least leave his daughters the substantial life insurance payout. Although he got his license to practice medicine back, his depression did not disappear. Lonely and isolated, he probably felt like a failure. If he had gone back into hospital because of his mental health problems, he might have lost his license forever.
1.1.4 Not Just the BrainBill's case not only shows how complex and multi-layered a human life can be. What is interesting for us now are the conclusions that Nancy Coover Andreasen drew from it for the biological revolution in psychiatry:
Psychiatry, like the prodigal son, has returned home to its place as a specialty within the field of medicine. It has become increasingly scientific and biological in its orientation. Psychiatry now recognizes that the serious mental illnesses are diseases in the same sense that cancer or high blood pressure are diseases. Mental illnesses are diseases that affect the brain, which is an organ of the body just as the heart or stomach is. People who suffer from mental illness suffer from a sick or broken brain, not from weak will, laziness, bad character, or bad upbringing. (Andreasen, 1984, p. 8)
According to the influential psychiatrist, the persecution of the “possessed,” the incarceration of patients such as James Norris or ultimately Bill's suicide would never have occurred if society had only correctly understood the nature of psychological-psychiatric disorders, namely as brain diseases. From this perspective, they would be seen in the same way as cancers: without shame, guilt and stigma. Then patients would be treated with more compassion, understanding and patience. More than 30 years later, Kenneth S. Kendler of Virginia Commonwealth University would argue that psychiatric disorders and psychiatry can only be taken seriously with a biological foundation (Kendler, 2016). Like Andreasen, he is an influential psychiatrist who sought to discover the biological basis of schizophrenia, primarily through genetic research, and helped shape some editions of the DSM.
From today's perspective, exactly 40 years later, we can look back on these far-reaching expectations, of which Andreasen was a relevant example. During these decades, Steven E. Hyman (1996–2001), Thomas R. Insel (2002–2015) and Joshua A. Gordon (since 2016), thus three neuropsychiatrists, were directors of the world-leading US National Institute of Mental Health (NIMH). Its director now decides on an annual budget of over 2.5 billion dollars, most of which is invested in research.Footnote 4 Gordon even described his field as “circuit psychiatry” when he was appointed, referring to neuronal circuits allegedly underlying mental disorders (Gordon, 2016). Rodents such as mice and rats are therefore an important model organism for psychiatric research. The perspective of human patients is scarce, just like with Meynert's approach in the nineteenth century.
When the DSM-5 was published in 2013, the disappointment was great: Not a single reliable diagnostic biomarker had been found for any of the several hundred mental disorders differentiated therein. Clinical psychologists and psychiatrists commonly still have to talk to their patients in order to make a diagnosis, and the mode of action of the frequently prescribed psychotropic drugs, for example for depression, is still very controversial (Davies et al., 2023; Moncrieff et al., 2023; Szasz, 1974; Valenstein, 1998). Experts from various disciplines have dealt intensively with this problem and possible reforms of psychiatry (Frances, 2013; Fuchs, 2018; Rose & Rose, 2023; Schleim, 2023; Scull, 2021). Thomas Insel commented on the progress made after his tenure as NIMH Director as follows:
I spent 13 years at NIMH really pushing on the neuroscience and genetics of mental disorders, and when I look back on that I realize that while I think I succeeded at getting lots of really cool papers published by cool scientists at fairly large costs – I think $20 billion – I don't think we moved the needle in reducing suicide, reducing hospitalizations, improving recovery for the tens of millions of people who have mental illness.Footnote 5
Like many others in the meantime, Insel now recommends a stronger focus on the prevention of mental disorders and on the social and institutional side of treatment (Insel, 2022). A decade earlier, he himself had explained to the general public that the disorders were caused by “faulty circuits” and had announced that “[n]euroscience is revealing the malfunctioning connections underlying psychological disorders and forcing psychiatrists to rethink the causes of mental illness” (Insel, 2010, p. 44). In the case of depression, for example, a certain brain region would have to be “rebooted,” as in the case of a crashed computer. Even if, to paraphrase Sperry, many things come together in the brain (Sperry, 1981), this central organ alone has not yet proven to be sufficient for understanding, let alone solving people's mental problems.
1.1.5 Psyche and SocietyThis brings us to the missing ingredient in understanding psychological-psychiatric disorders: Factors such as poverty, stress, relationship status, living in a city, severe life events, workplace organization, and the availability of help all play an important role in our mental health (Arango et al., 2021; Mirowsky & Ross, 2003; OECD, 2011; Rugulies et al, 2023; Sheldon et al, 2021; WHO, 2004). If we take another look at Bill's life from this perspective, the problem may look quite different:
In his biography, a combination of outstanding achievements and high functional pressure stands out. When his father died, he wanted (or was supposed) to resume and complete his studies after just one month. Having to repeat the last year was a humiliation for him. The extent to which grief after the loss of a loved one is normal or a characteristic of a depressive disorder has long been disputed (Frances, 2013). In the past, the therapist or psychiatrist played a decisive role in drawing these boundaries: They were supposed to assess the extent to which the grief conformed to cultural norms.
The DSM-5-TR of 2022 recently added “prolonged grief disorder” as a new category. Intense loneliness, experienced meaninglessness of life, intense emotional pain and dysfunction in everyday life are exemplary symptoms (APA, 2022). A mourning period of one year is considered normal for adults and six months for children and adolescents. Bill had only taken a fraction of this time for himself. Even after the death of his wife and the divorce, the pressure to function, this time as a doctor with his own practice, had always remained very high.
Another striking feature is the strong social rejection of mental health problems or their stigmatization in his environment. In part, this could be seen as the flip side of the pressure to function: Bill had no choice but to continue studying or working quickly because that was the only thing that was considered acceptable. He also didn't seem to be able to talk to friends or family about his feelings and fears. This was perhaps all linked to a certain ideal of masculinity that was particularly strong for the socially respected but also responsible role of a doctor. Andreasen explicitly described how he was expected to have more self-control and resilience.
Even decades later, the significantly higher suicide rate among men was explained by certain ideas of masculinity (Swami et al., 2008). The tendency of members of this gender to be unable to talk about their feelings (Chandler, 2022) is cited as an important factor, as is a certain understanding of heroism (Rasmussen et al., 2018). We remember the idea of sacrificing oneself so that one's daughters receive the high life insurance premium. Such psychosocial explanations were not considered for a long time because many researchers believed that the large gender difference in suicide rates had to be explained genetically (Swami et al., 2008).
The holistic view adopted by myself and others does not deny that Bill was also a biological being with a certain genetic disposition, a nervous system and a brain. However, considerable doubts are raised as to whether the problem—and therefore the solution—can be found primarily at this level. Even though psychotropic drugs and later the stimulation of his brain with a strong electrical current improved the symptoms, these interventions did nothing to change the inner and outer harshness and rejection that Bill had to deal with after the heavy blows of fate. In psychotherapy, the internalized thought patterns could have been questioned and thus perhaps gradually changed; and according to the social psychiatric approach, he could perhaps have been provided with an assistant for the practice or found an environment with less functional pressure.
Andreasen ends the introduction to her book with the remark that a better—by which she meant: biological—understanding of mental disorders unfortunately came too late for Bill (Andreasen,
Comments (0)