The SMARCA4gene on chromosome 19p13 encodes the transcription activator BRG1, which is pivotal in regulating transcriptional processes in various cancers [18]. As an ATP-dependent catalytic subunit of the SWI/SNF complex, SMARCA4 provides the energy required for chromatin remodeling through its ATPase enzymatic function [18]. The 2021 WHO Classification of Thoracic Tumors (5th edition) recognizes SMARCA4-dNSCLC as a distinct entity within thoracic tumors [19]. Histologically, SMARCA4-dNSCLC can present as differentiated adenocarcinoma, squamous carcinoma, or undifferentiated carcinoma [16]. Most patients are diagnosed at stage IV, which is characterized by aggressive tumor behavior, high Ki-67 indices, and a significant incidence of adrenal and lymph node metastases [10, 12, 13, 20].
A recent study on SMARCA4-dNSCLC reported that the majority of cases involved chronic smokers aged 48–83 years (median age: 67), with a male-to-female ratio of 34:1 [12]. Our case is consistent with these findings, involving a middle-aged male with a 40-year history of heavy smoking.
Patients with SMARCA4-dNSCLC often exhibit nonspecific symptoms similar to other types of lung cancer, including cough, dyspnea, chest pain, hoarseness, and hemoptysis [21, 22]. However, a study by Kim et al. found that only one patient (11.1%) exhibited symptoms such as hoarseness, cough, and sputum at diagnosis, while the remaining eight (88.9%) were asymptomatic [23]. Gastrointestinal metastases from primary lung cancer [24], are symptomatic in only 0.2% to 1.7% of patients. They are rare and sometimes misdiagnosed as primary digestive tract tumors [7, 8]. Common initial symptoms of colonic metastases include abdominal pain due to intestinal obstruction, melena, or hematochezia [5, 25,26,27,28], although some gastrointestinal metastases remain asymptomatic in the early stages. In our case, the patient initially exhibited no intestinal symptoms, although a fecal occult blood test was positive and CT imaging revealed colonic carcinoma (confirmed via colonoscopy). The patient later developed melena as the carcinoma progressed. The low incidence and lack of characteristic symptoms make the initial diagnosis of colonic metastasis from lung cancer particularly challenging.
Histological examination remains the gold standard for diagnosing SMARCA4-dNSCLC. Immunohistochemistry (IHC) and molecular analyses are crucial in distinguishing SMARCA4-dNSCLC from other similar tumors. These tumors typically test negative for BRG-1 and TTF-1 but positive for CK7 [10, 12]. In our patient, the lung lesion was CK7-positive and BRG-1- and TTF-1-negative, confirming SMARCA4-dNSCLC. IHC aids in determining the tumor’s primary origin. The CK20⁻/CK7⁺ phenotype is predominant in non-mucinous ovarian, breast, thyroid, kidney, endometrial, pancreatic, and lung adenocarcinomas, as well as in mesotheliomas. It is also observed in over 50% of non-colorectal gastrointestinal tract (GIT) adenocarcinomas. CK20 is primarily expressed in tumors of gastrointestinal origin, urothelial carcinomas, and Merkel cell carcinomas, whereas CK7 is expressed in a broader range of tumors but is typically negative in colorectal and prostate adenocarcinomas [29]. CK18 and CK19 are widely expressed in carcinomas of the breast, prostate, lung, colon, and ovary [30]. Notably, CK19 shows high expression in prostatic adenocarcinoma (PAC), with levels increasing significantly as the Gleason grade group advances [31]. Additionally, CDX2 serves as an important marker for tumors of gastrointestinal origin [32]. In this case, the sigmoid colon tumor was positive for CK7, and negative for TTF-1, CDX2, and CK20, confirming metastatic colon cancer originating from SMARCA4-dNSCLC.
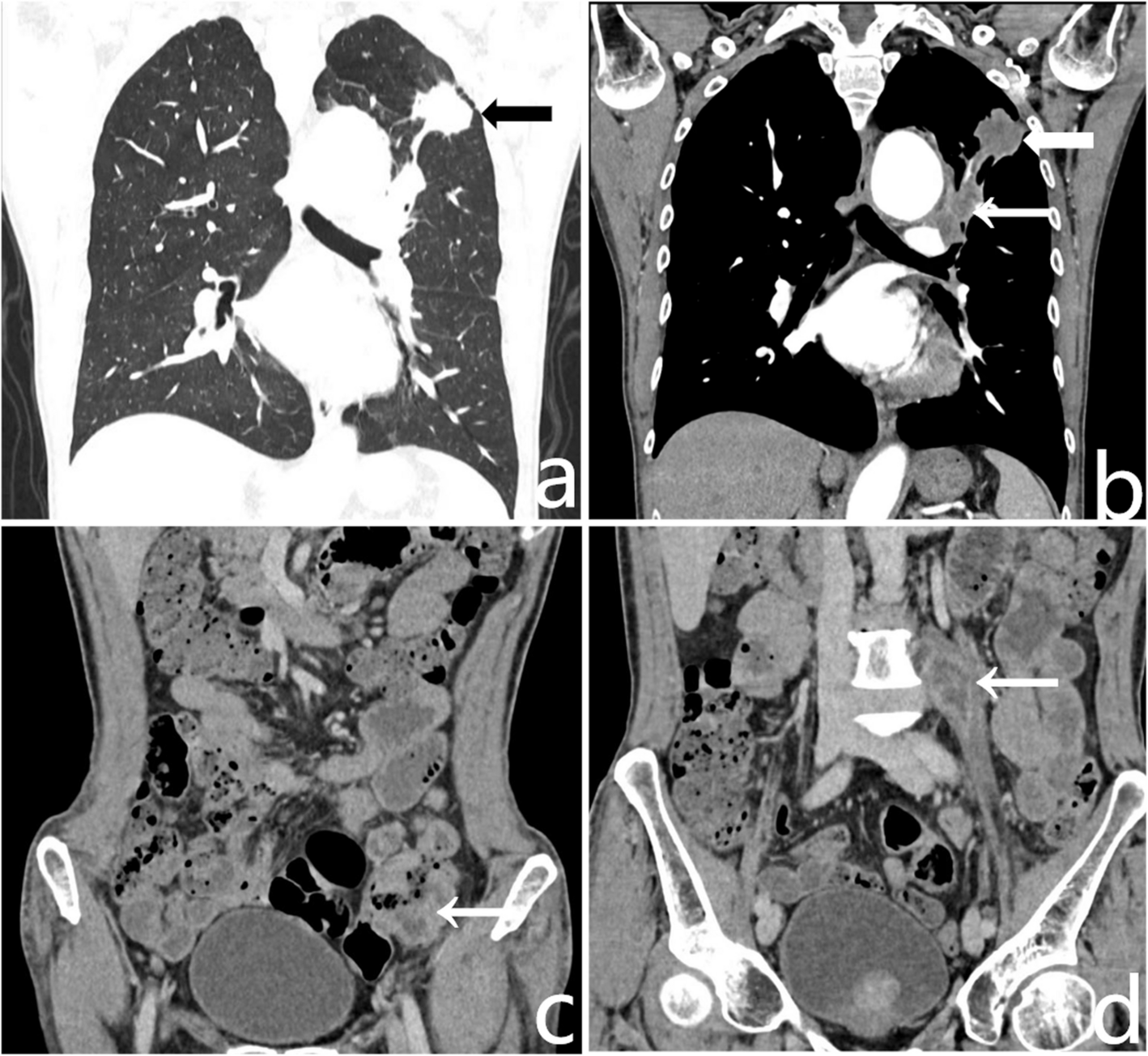
The imaging features of SMARCA4-dNSCLC have been described in limited studies. These tumors typically appear as primary solid lung masses on CT, often located in the upper lobe and periphery of the lung [12, 15]. Unlike general ground-glass opacities, the mass diameter remains consistent across lung and mediastinal windows. The tumors rarely exhibit benign calcification but may show vascular convergence, cavitation, speculation, and pleural invasion. Tumor sizes range from 14.16 mm to 92.25 mm and are more likely to metastasize within the lung than other NSCLC types [15]. Our case presented with an irregularly shaped mass in the left lung’s upper lobe, consistent with prior reports, showing heterogeneous contrast enhancement, spiculation, lobulation, pleural retraction, and enlarged mediastinal and hilar lymph nodes.
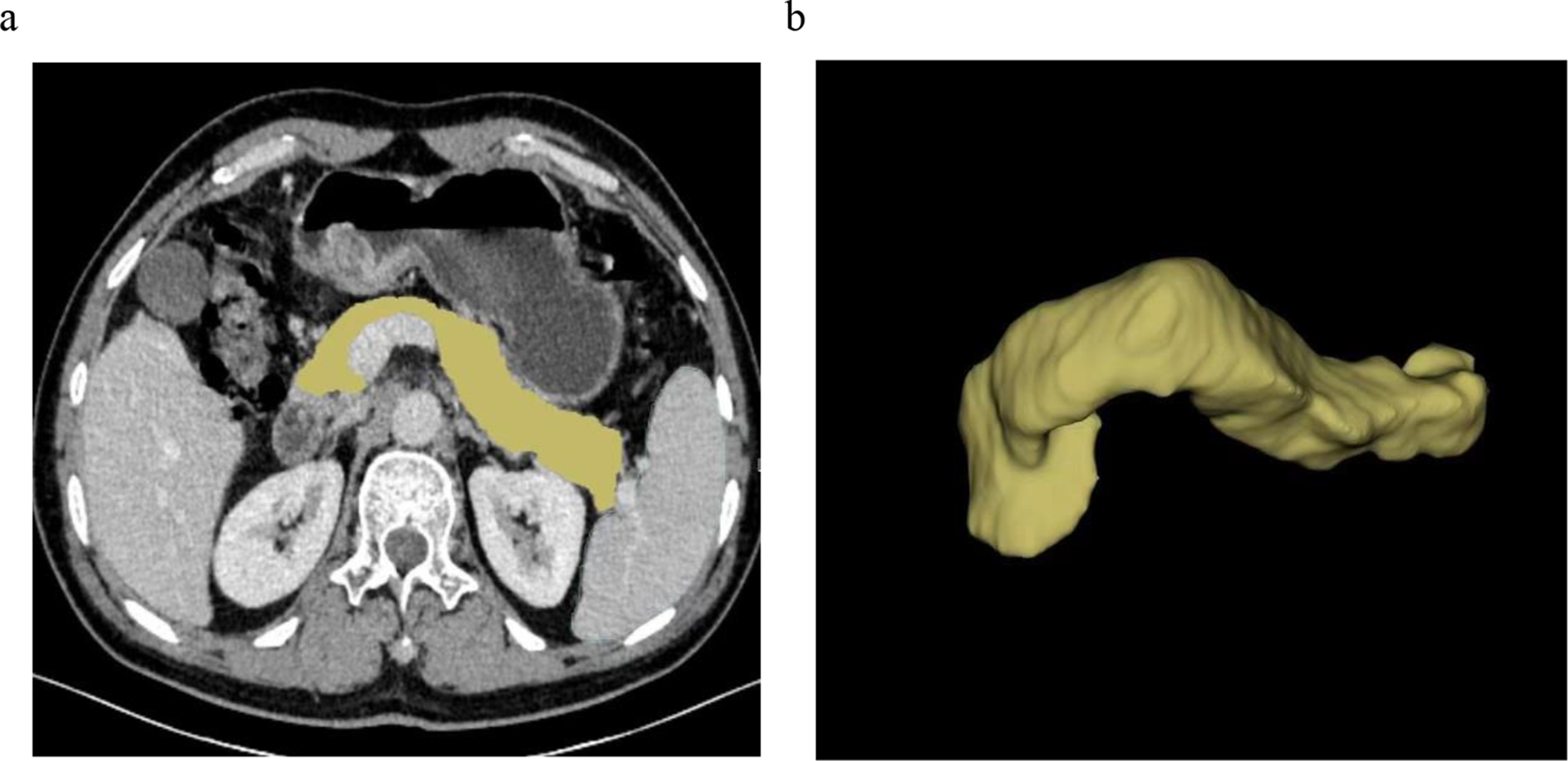
Colonic metastases from primary lung cancer are rare, and the CT features of gastrointestinal metastases remain underexplored. According to Kim et al., these metastases typically appear as a short segmental bowel-wall thickening or intraluminal polypoid masses with isoattenuating enhancement patterns [7]. These lesions may be accompanied by mild regional lymphadenopathy. Primary adenocarcinoma often results in intestinal lumen stenosis, whereas gastrointestinal metastases from lung cancer rarely lead to intestinal obstruction unless intussusception occurs [7]. In our patient, abdominal CT revealed uneven thickening of the sigmoid colon wall without obstruction but with lymphadenopathy anterior to the left psoas major muscle, consistent with previously reported features. Due to the lack of specificity from imaging and rarity of the disease, distinguishing intestinal metastases from primary intestinal tumors remains challenging. In our case, the definite diagnosis of metastatic colon carcinoma was only made after surgery. Lymph node and distant metastases are common in patients with SMARCA4-dNSCLC [15]. In previous case reports, all patients presented with primary pulmonary nodules or masses alongside multiple metastatic lesions involving the bones, adrenal glands, liver, brain, and lymph nodes [19, 33, 34], but none involved the gastrointestinal tract. Our case was the first 1 showing metastasis to the colon from SMARCA4-dNSCLC. At diagnosis, our patient exhibited mediastinal and retroperitoneal lymph node metastases, as well as sigmoid colon metastases, highlighting the high invasiveness of SMARCA4-dNSCLC. In Table 2, we summarize previously reported cases of SMARCA4—dNSCLC.
Table 2 The previously reported cases of SMARCA4-dNSCLCIn addition, whole positron emission tomography—CT (PET-CT) is valuable for assessing disease burden and treatment response in SMARCA4-dNSCLC. It is widely used in diagnosing gastrointestinal tract metastatic tumors, demonstrating high sensitivity and specificity [26]. The study by Wumener X et al. showed that the rate constant (Ki) of metastatic lymph nodes in lung cancer was significantly higher than that of non-metastatic lymph nodes [34]. PET scanning detects extrathoracic metastases in approximately 25% of patients with clinical stage III disease and may reveal a higher incidence of colonic metastases than previously recognized [36]. In a stage IV SMARCA4—dNSCLC patient, PET-CT after 48 cycles of pembrolizumab treatment demonstrated complete resolution of uptake in all lesions [33]. In another case, post-treatment PET-CT revealed a marked reduction in FDG uptake in the primary lung lesion, with the maximum standardized uptake value (SUVmax) decreasing from 22.4 to 2.2 [34].
The differential diagnosis of SMARCA4-dNSCLC includes SMARCA4-deficient undifferentiated tumor (SMARCA4-UT)and small cell lung cancer (SCLC). Similar to SMARCA4-dNSCLC, SMARCA4-UT also belongs to the category of SMARCA4-deficient tumors. However, SMARCA4-UT is distinguished by more prominent tumor necrosis, with infiltration and compression of surrounding tissues and necrotizing lymphadenopathy, which helps differentiate it from SMARCA4-dNSCLC [37]. SCLC, another highly invasive malignancy of the chest, typically presents as a centrally located lung mass with mediastinal lymph node enlargement. Characteristically, SCLC involves central airway infiltration of the submucosal layer, leading to progressive narrowing of the bronchial lumen through outward or endobronchial spread [38]. These features further differentiate SCLC from the current case.
Compared with other types of lung cancer, SMARCA4-dNSCLC is highly invasive and has a poor response to conventional chemotherapy [18]. A study reported that the median overall survival (mOS) for patients with SMARCA4-dNSCLC is 12.2 months, with a 1-year survival rate of 51% and a 2-year survival rate of 20% [12]. In patients with stage IV disease, the median survival was significantly shortened to 4.4 months compared with those with stage II/III disease [11]. Studies have demonstrated the efficacy of ICIs in treating SMARCA4-dNSCLC [13]. Tomoyuki N. et al. reported a case in which a patient with SMARCA4-dNSCLC exhibited a sustained response to fourth-line nivolumab therapy for 14 months [39]. Notably, patients with advanced SMARCA4-dNSCLC show improved mOS when treated with a combination of immune checkpoint inhibitors and chemotherapy [12].
In addition, targeted therapies show promise in treating SMARCA4-dNSCLC. Preclinical studies and ongoing clinical trials suggest potential efficacy of inhibitors targeting oxidative phosphorylation (OXPHOS), aurora kinase A (AURKA), ataxia telangiectasia and Rad3-related (ATR), EZH2, and cyclin-dependent kinase 4/6 (CDK4/6) [18]. Palbociclib, a CDK4/6 inhibitor, effectively suppresses tumor growth in SMARCA4-mutant NSCLC xenograft models. IHC analysis revealed significant reductions in RB phosphorylation, Ki67 expression, and the mitotic index following palbociclib treatment [40]. Recent studies have identified polycomb repressive complex 2 (PRC2) as a potential therapeutic target for the topoisomerase II (TopoII) inhibitor etoposide, which has shown survival benefits in NSCLC patients. The OXPHOS inhibitor IACS-010759, currently in clinical development, has shown potent antitumor efficacy and a favorable safety profile in SMARCA4-deficient NSCLC cell lines [18]. However, further clinical trials are needed to validate these targeted therapies and optimize their clinical benefits for advanced SMARCA4-dNSCLC.
However, the prognosis for primary lung cancer with intestinal metastasis is poor. Survival times following the discovery of colonic metastases from primary lung cancer typically range from 5 weeks to 1 year, with most patients succumbing within 6 months [24]. Patients receiving palliative surgical resection of the metastatic lesion showed a longer survival time [25, 41]. One report described a lung cancer patient who survived for more than 5 years after surgical resection of metastatic intestinal lesions [42]. Although patients with gastrointestinal metastasis from lung cancer were in the advanced stage of the disease, surgical intervention for colonic metastasis may offer symptomatic relief and clinical benefit. In our case, the patient underwent surgical resection of the sigmoid colon metastasis and continued treatment with nedaplatin combined with bevacizumab and camrelizumab after surgery. Although metastasis to the left adrenal gland was discovered 2 months post-surgery, the patient's general condition remained stable, and the primary pulmonary mass responded well to treatment.







Comments (0)