A hands-free wearable electrolarynx for communication in tracheostomized mechanically ventilated critically ill patients: a case series
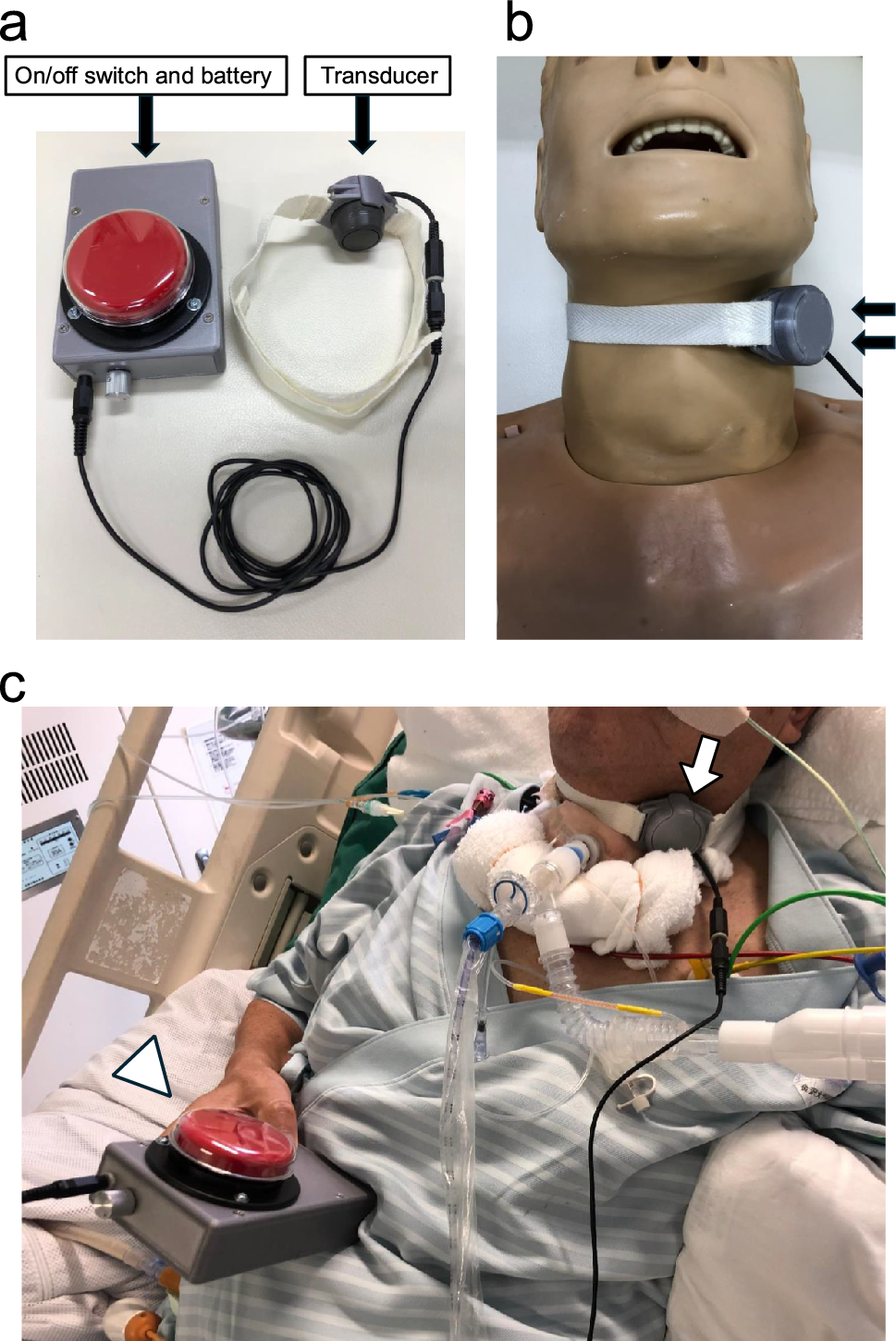
One of the principal factors contributing to effective communication in critically ill patients with artificial airways is the ability to achieve independent communication [7]. Independent electrolarynx use typically depends on adequate muscle strength to hold and securely position the device. Improper contact with the neck and surrounding tissues may produce radiated noise, potentially compromising speech intelligibility [8]. Sedation level can also influence training effectiveness. Rose et al. [4] reported that user-friendliness and the capacity for independent use facilitated the utilization of the electrolarynx among critically ill patients. Once the hands-free electrolarynx transducer was placed on the patient’s neck, some were able to produce intelligible speech independently, demonstrating their ability to autonomously initiate conversations. Although the EES of the hands-free electrolarynx were comparable to those of the conventional electrolarynx with assistance, the hands-free device may support greater patient independence in communication.
One patient experienced decreased oxygen saturation due to increased coughing during phonation using the hands-free electrolarynx. This patient (Case 4) had the worst oxygenation capacity, characterized by excessive sputum production due to pneumonia. Theoretically, the respiratory cycle was independent during electrolarynx speech because it did not rely on airflow. However, mechanically ventilated patients often either exhaled or stopped breathing temporarily during phonation using the electrolarynx, with most patients using the pressure support mode to regulate the respiratory cycle better. For patients with low respiratory reserve, synchronizing their breathing cycle with speech is particularly challenging. In addition, speech using the electrolarynx requires precise, exaggerated mouth movements and slow articulation for optimal intelligibility, which may further contribute to patient ventilator desynchrony in this patient population [9]. Further research is necessary to explore the link between respiratory status and complications arising from electrolarynx use.
This study has several limitations. First, the small sample size due to the limited number of eligible patients may reduce the generalizability of our findings. Although our findings suggest potential clinical advantages of the hands-free wearable electrolarynx, further large-scale studies are necessary to comprehensively evaluate its effectiveness and broader clinical applicability. Second, the duration of electrolarynx use in this study was short, and the long-term feasibility and safety of the device needed to be evaluated. Third, the devices were not blinded to the raters, which could have introduced bias in the assessment process. Moreover, the experienced research team assisted in using the conventional electrolarynx, which may have influenced the comparison between the devices. The learning curve and user adaptability of the hands-free electrolarynx were not fully evaluated in this study. Further research is needed to quantify the time required for users to become proficient and to assess how usability evolves with experience. Furthermore, the EES evaluation was perceptual and reliant on subjective judgment. Finally, the study was conducted at a single center in Japan with only native Japanese speakers, which may limit the generalizability of our findings to populations speaking other languages or to different clinical settings.
In conclusion, our case series provides preliminary evidence indicating the feasibility of using a hands-free electrolarynx for communication in tracheostomized, mechanically ventilated patients. When used independently by patients, the hands-free electrolarynx achieved greater intelligibility than the conventional electrolarynx. This device may reduce the need for external assistance, potentially enhancing effective communication with medical staff and family members.




Comments (0)