Study and Patient Characteristics
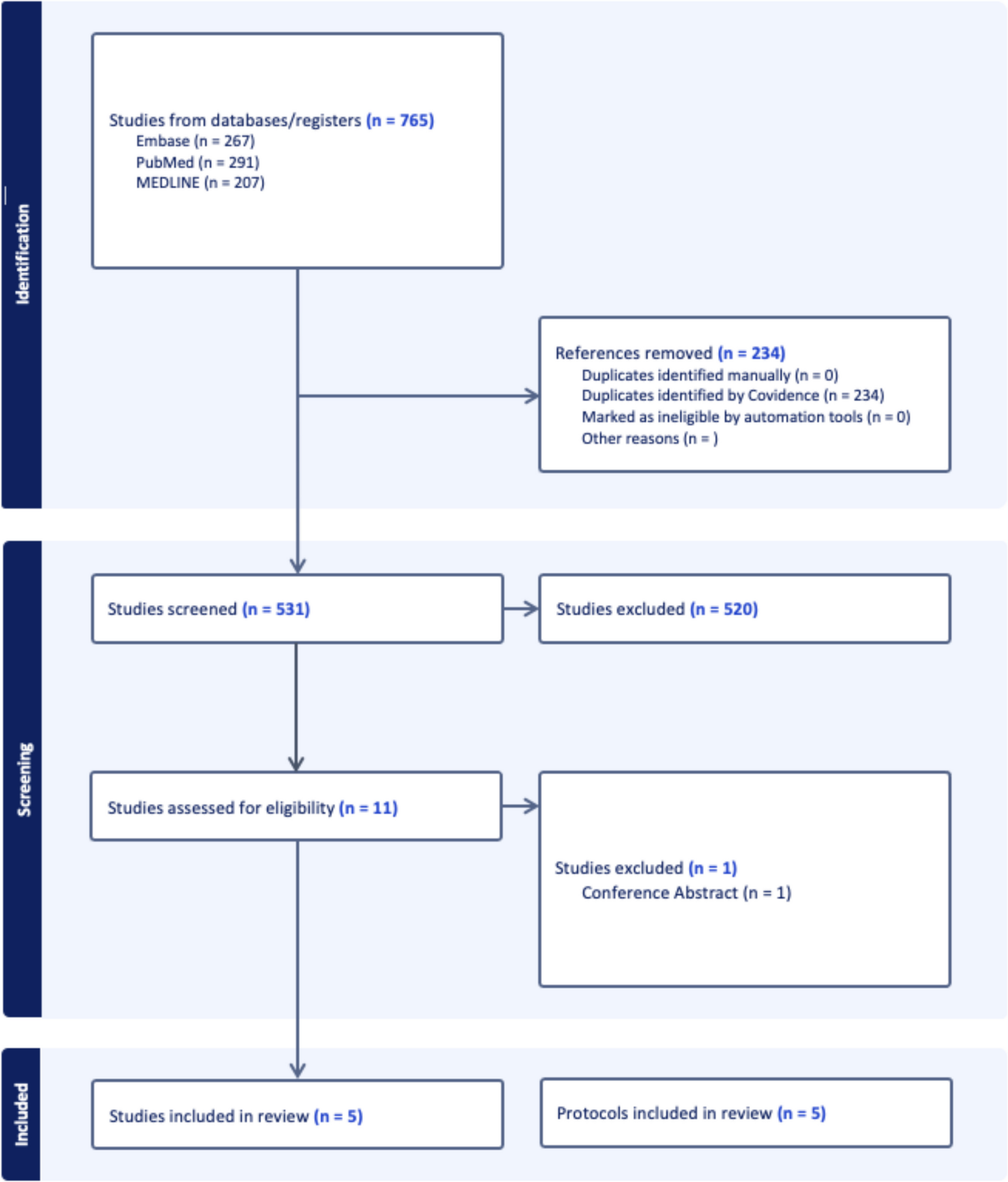
Five studies [14,15,16,17,18] have been included in this review, with 368 patients in total. Two studies were RCTs [14, 18] and the three others [15,16,17] were prospective cohort studies. Three studies recruited only symptomatic patients postoperatively [14,15,16], while the two most recently published studies [17, 18] recruited all patients undergoing low anterior resection preoperatively.
Study sample sizes ranged from 8 to 137 patients. The mean age of patients was 63 years. In terms of risk factors for LARS, neoadjuvant therapy was given to 48% of patients in the four studies that reported its use, 64.4% of patients had a diverting stoma and the median timing of stoma closure ranged from 72 days to 20 months. All studies were assessed to have an overall low risk of bias. A summary of the included studies which have already been performed is shown in Table 1.
Table 1 Characteristics of included studies with dataGiven the small number of studies available, five protocols of future studies [19,20,21,22,23] related to education for LARS patients have been included for analysis of content and method of delivery. Three of these studies recruit all patients undergoing low anterior resection either preoperatively or prior to their ostomy reversal, while the other two recruit patients symptomatic with LARS postoperatively. This may reflect a contemporary trend towards an increasingly proactive approach to healthcare and intervention.
Delivery and Contents of Education Intervention
The majority of education interventions were delivered in the postoperative period after sphincter-preserving surgery or ileostomy closure; only the study by Harji [15] introduced the education intervention in the preoperative period. Education was delivered in multiple methods, including in-person sessions that were either individual or in groups, phone reviews and online modules. In future study protocols, a specific information booklet for LARS and online and phone applications are being produced for RCTs [19,20,21,22,23]. The contents of the education interventions mainly included advice on dietary changes and toileting habits that are used to manage LARS, detailed information about LARS itself and the functional outcomes that can be expected postoperatively, as well as disease experience of other similar patients [14,15,16,17,18]. The length of the education intervention varied, ranging from 2 to 12 months after the initial operation. A summary of the education interventions and follow-up is shown in Table 2.
Table 2 Summary of education interventionsComparison and Co-interventions
In the included RCTs, the control groups received standard care, which included the education intervention, while the intervention groups received pelvic floor muscle training (PFMT) alongside standard care [14, 18]. In two of the prospective cohort studies [15, 16], patients received stepwise care depending on the severity and response of their symptoms, starting from educational intervention only, then medications, PFMT and transanal irrigation (TAI), and finally surgical intervention. In future RCTs, online and phone applications will be compared to a standard written information booklet for LARS [19,20,21,22,23].
Impact on LARS
Four of the five included studies [14,15,16, 18] described the impact of their interventions on LARS. Van der Heijden et al. [14] reported no significant difference in the change of LARS score in the pelvic floor rehabilitation (PFR) group compared to standard care (mean difference: PFR − 2.4 vs. control − 2.3, p = 0.93). Kim et al. [18] reported an average difference in LARS score of − 2.28 in the intervention group compared to the control group, and a lower prevalence of major LARS in the intervention group at 3 months (52.4% vs. 71.4%). Harji et al. [15] reported that with their rehabilitation programme, the prevalence of major LARS decreased from 48 to 12%, and the prevalence of Wexner score > 4 decreased from 59 to 22% in 12 months. Seventy-seven percent of patients from Harji’s cohort only required education and anti-diarrhoeal drugs to improve their LARS symptoms during the 12-month follow-up period. Dalsgaard et al. [16] reported that 51.2% of their patients required basic treatment, i.e. education and medications only, and within this group, the prevalence of major LARS decreased from 97 to 57%.
Quality of Life
Quality of life measures were reported by three studies [14, 15, 18]. The two RCTs used the European Organisation of Research and Treatment of Cancer (EORTC QLQ-CR29) questionnaire to assess quality of life, while Harji et al. used the EQ-5D questionnaire. Van der Heijden et al. [14] reported no significant difference between the two groups in the final EORTC scores, but there was a clinical difference in favour of the intervention group in relevant domains such as anxiety and urinary frequency. Kim et al. [17] also reported no significant differences between the two groups in all functional and symptom scores of the EORTC questionnaire, except for lower abdominal pain scores in the intervention group. Harji et al.’s study [15] only measured quality of life at the end of follow-up and found no difference in EQ-5D questionnaire scores between patients with major or minor LARS.
Olivia et al.’s study [17] reported descriptive outcomes after implementing their online educational modules for LARS. Their participants described that the online educational module provided credible information on LARS, which was delivered at an appropriate reading level and had useful accompanying illustrations. The patient forum on the online module allowed participants to share their own experiences and provide emotional support to one another. A satisfaction survey was provided at the end of their follow-up, and seven of the eight participants were ‘mostly’ or ‘very’ satisfied with the information provided by the online educational modules, and all eight participants would recommend it to other rectal cancer survivors with LARS.





Comments (0)