
Remember me




The study team selected 10 Local Government Areas (LGAs) in Sokoto and stratified the LGAs to represent each of the three senatorial zones in the state, with a mix of urban and rural areas and high- and low-performing LGAs based on their reported vaccination coverage rates. LGAs receiving substantial RI program support from partner agencies beyond support sponsored through the partnership with the Bill & Melinda Gates Foundation, the Dangote Foundation and USAID were not included in the sample to minimize bias and contamination (MCSP 2018). LGAs facing security challenges were not included in the sample to protect the safety of data collectors. LGAs in each zone were randomly assigned to intervention and comparison groups.
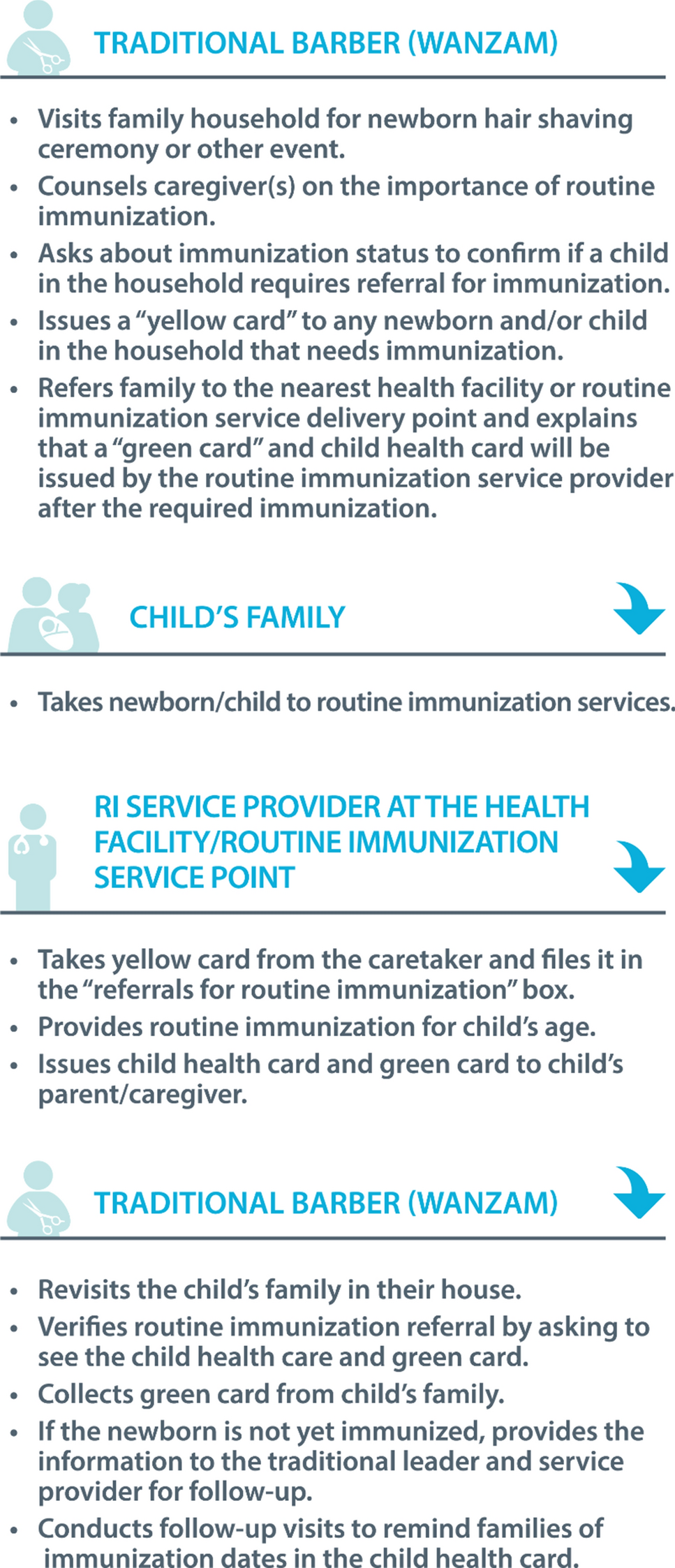
Intervention descriptionThe Maternal and Child Survival Program (MCSP), funded by the US Agency for International Development (USAID) worked closely with the SPHDCA throughout 2018 to engage with traditional authorities. In northern Nigeria, traditional authorities became an important partner in the Polio Eradication Initiative after the Sultan of Sokoto, a Muslim spiritual leader, publicly announced his support for the initiative (Nasir et al. 2014). The traditional authorities operate within a hierarchical structure from the state down to the community level where they engage directly with community leaders and traditional barbers’ associations. The MCSP supported the SPHCDA in May 2018 to train 1210 traditional barbers who were selected by traditional authorities along with orienting health providers and community leaders in five LGAs in Sokoto to identify and refer newborns for RI; 844 barbers participated in the strategy. The barber’s training included the importance of immunization, how to counsel and educate a family about the benefit of immunization through interpersonal communication and the process of using color-coded referral cards. SPHCDA encouraged traditional barbers to re-visit the family once to confirm compliance with the vaccination referral. However, this visit was not mandated since the traditional barber was not provided with an incentive to repeat visits. There were no follow-up trainings or direct supervision provided to the traditional barbers. However, monthly meetings facilitated by health providers with traditional barbers and community representatives provided an opportunity for questions and feedback and traditional barbers were encouraged to report defaulters to community leaders. SPHCDA program managers also monitored the number of each color card distributed and recovered each month. The steps involved in the approach are described in Fig. 1.
Fig. 1
Outline of steps in newborn tracking approach, Nigeria 2017–2018
Figure 2 presents a Theory of Change (ToC) that describes how the strategy was expected to influence immunization coverage. The strategy is grounded in the Health Belief Model, which recognizes that parents will be more likely to vaccinate their child if they understand that the vaccine-preventable illness is serious, that their child is susceptible and that there is an increased threat to their child if they are not immunized (Murele et al. 2014; Rosenstock 1974). The strategy uses the traditional barber to provide information and a cue to action for parents to initiate the use of RI services, grounded in an understanding that social relationships within the community have a strong influence on health behaviors (Ataguba et al. 2016). These relationships can help to mitigate some of the socio-demographic factors that affect immunization coverage (Ataguba et al. 2016; Adenike et al. 2017; Sibeudu et al. 2017).
Fig. 2
Theory of change for using traditional barbers to identify, and refer newborns for routine immunization services, Nigeria 2017–2018
Study designThe mixed methods study included quantitative methods to assess differential changes over time in immunization coverage rates associated with the strategy, while explaining how and why changes occurred using qualitative methods.
QuantitativeThe study team administered a pre/post-quasi-experimental survey with the baseline survey implemented before program implementation in December 2017 and the endline survey administered at the conclusion of implementation in October to November 2018.
We used a two-stage stratified sampling procedure. In the first stage, we listed all enumeration areas by ward in each of the 10 selected LGAs. We then used probability proportion to size to select 60 enumeration areas per LGA starting at a random point and then systematically selecting areas using a fixed sampling interval. In total, we sampled 300 enumeration areas for each study group. In the second stage, the study team enumerated all households and screened the household for eligible women. We randomly selected ten households per enumeration area and interviewed 10 women between 15 and 49 years of age who had been married and had a child under the age of 2 years. Individuals under the age of 18 are considered emancipated if they are married or in union. In these instances, verbal consent from the participant was obtained without guardian consent.
We selected women who had a child between 0 and 23 months because this enabled us to follow children who were born during the intervention period and who would have had up to 6 months of exposure to the traditional barber intervention. We estimated a sample size of 1300 children between the ages of 0-5 months per survey area, totaling 2600 children for the two survey areas at baseline and at endline. This sample size was based on a change of 5% points in the proportion of infants 0–5 months receiving BCG at birth in the intervention area, with 80% power to detect a difference, alpha of 0.05 and assumptions of an intracluster correlation of 0.21, determined from DHS data (Lê and Verma 1997) and a 10% non-response rate.
The principal outcomes of the survey were birth antigens including the proportion of infants 0–5 months who received the birth doses of oral polio vaccine (OPV), BCG and hepatitis B (HepB) vaccines. We measured OPV and BCG doses based on data recorded from the child’s vaccination card, and when a vaccination card was not available, the information was based on the mother’s recall. Hepatitis B vaccine was based only on data recorded on the child’s vaccination card. We also collected additional socio-demographic information including household assets (to compute a wealth index following DHS methods (Rutstein and Johnson 2004)), residence, sex of the child and maternal characteristics, such as parity, age and education. We measured changes in knowledge and attitudes related to vaccines. Finally, we assessed exposure to the program by measuring the percent of mothers who received a yellow referral card from a traditional barber during the implementation period.
QualitativeThe qualitative component of the study included focus group discussions (FGD) and in-depth interviews (IDIs). We conducted interviews at the state level and in a subset of three intervention LGAs (i.e., Dange Shuni, Illela, Shagari) in September 2018, interviewing 18 respondents who were involved in the development and implementation of the strategy. The study team conducted two FGDs with parents who had an infant born in the year preceding the interview (mothers and fathers were interviewed separately), two FGDs with ward development committee members and one FGD with traditional barbers in each of the three LGAs, for a total of 21 FGDs. The study team also conducted four IDIs with village heads and five health providers from each LGA for a total of 27 IDIs at the community level. The study team worked with government and community representatives to purposively select respondents to achieve a geographic mix of individuals involved in or exposed to the program’s intervention. Moderators conducted the interviews with community members in the local language of Hausa. Interviews were recorded using a digital audio recorder and translated and transcribed into English.
AnalysisTo measure the effect of the program, we estimated simple logistic regression models on each birth antigen while controlling for demographic characteristics using Stata SE 15. Variables were selected for inclusion in an adjusted logistic regression model if they satisfied the criterion of p < 0.05 in the simple logistic regression model. To assess the effect of the program, we controlled for the study period (baseline and endline) and study group. We also included a measure to assess whether the respondent had received a yellow referral card from a traditional barber to measure the effect of program exposure. We performed diagnostic tests to check for specification errors, goodness of fit and collinearity with the regression models. We accounted for the design effect by assigning the enumeration areas as the primary sampling unit for analysis.
We used thematic analysis techniques to identify themes emerging from the qualitative data. We considered how traditional barbers influence caregiver decisions to seek immunization services and explored the challenges and opportunities associated with engaging traditional barbers to refer newborns for immunization services. We used the ToC model to develop codes related to how the intervention influenced the outcomes such as parental knowledge and identified emerging themes to code challenges (e.g., the need for incentives) and enabling factors (e.g., traditional leader support). We applied the codes in Nvivo 12. Findings were described and compared across subgroups. We used findings from the qualitative data to contextualize the quantitative data to develop a more comprehensive understanding of how the program was implemented and what factors related to the context and implementation influenced the results.
Comments (0)