The incidence of perioperative complications in adrenalectomy is reported to range from 1.7 to 30.7% [16, 17]. To predict the risk of complications after adrenalectomy, the PACS (Arterial pressure, surgical approach, catecholamine level, sex) risk score and the National Surgical Quality Improvement Program (NSQIP) risk calculator have been successfully utilized. In addition, various nomograms have been developed [8,9,10]. Although various risk calculators and nomograms are used to predict adrenalectomy complications, these studies have primarily focused on specific surgical types or adrenal lesions [9, 10]. Additionally, while various predictive models for adrenalectomy exist in the literature, it has been observed that they do not thoroughly examine preoperative and intraoperative factors. The E-PASS scoring system comprehensively evaluates multiple preoperative and intraoperative factors, enabling the early prediction of complications in the immediate postoperative period [14].
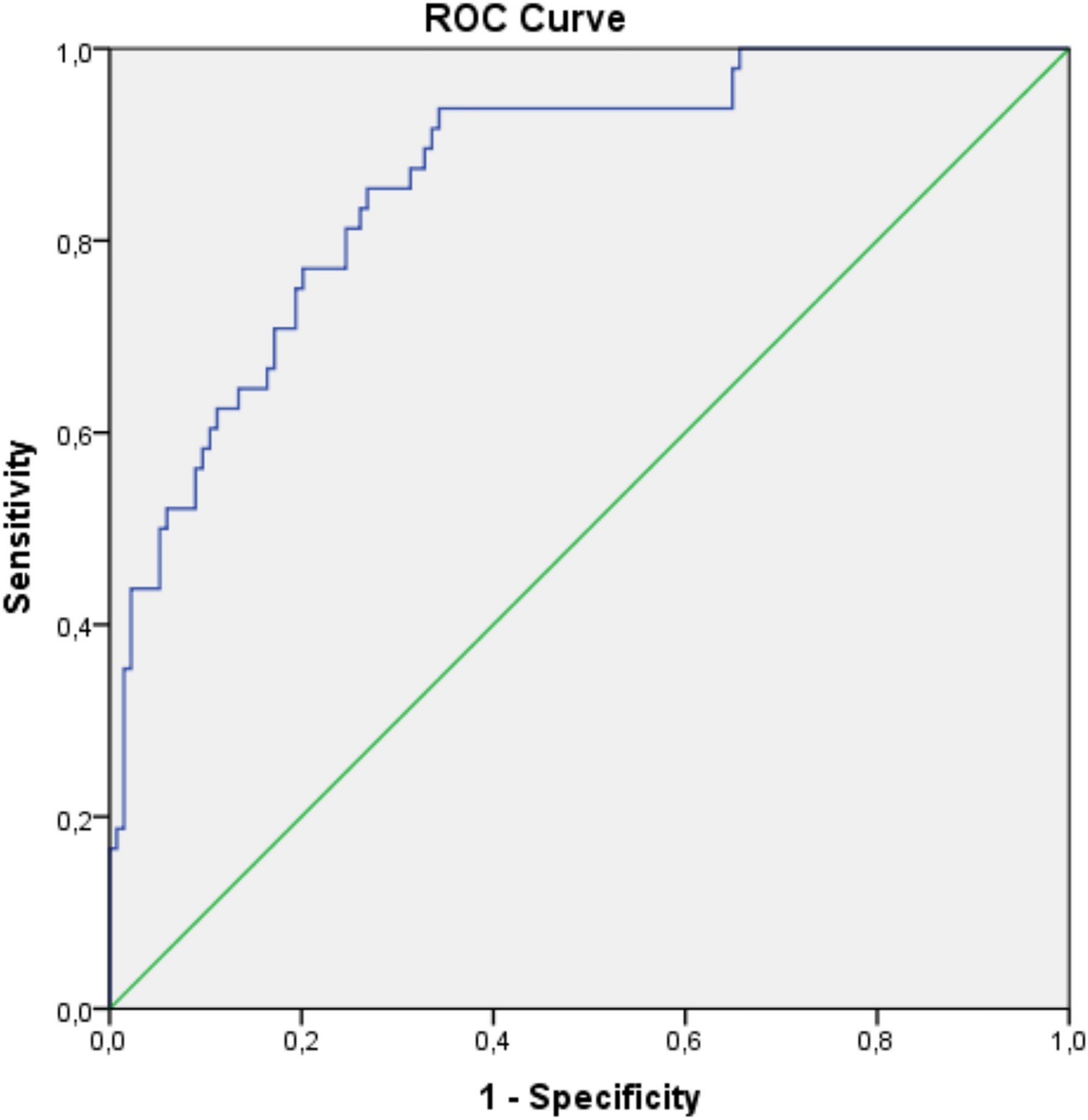
The E-PASS scoring system has been successfully applied in surgeries across various surgical specialties [12,13,14, 18, 19]. Kondo et al. reported that an E-PASS CRS > − 0.058 is associated with an elevated risk of postoperative complications in colorectal surgeries [18]. Additionally, it has been found that the E-PASS scoring system can successfully predict complications in spinal surgery and acetabular fracture surgery [12, 19]. In the literature, there are two studies that investigate the use of E-PASS in urological surgery [13, 14]. In the study involving 252 patients undergoing radical cystectomy and ileal loop surgery, the cut-off value for the CRS predicting postoperative complications was established at 0.4911 [14]. Additionally, a study has been conducted on laparoscopic nephrectomy. According to the findings of this research, the CRS > − 0.2996 is associated with a 2.8 times increase in the risk of postoperative complications [13]. This study is the first in the literature to examine adrenalectomy and it found that an E-PASS CRS score > − 0.0677 was identified as an independent risk factor for postoperative complication.
Surogi et al. examined the complication rates in 154 cases of OA and LA. The total complication rate was 26%, with complications distributed as 67.5% in Grade I and Grade II, 15% in Grade IIIa, 7.5% in Grade IIIb, 0% in Grade IV and 10% in Grade V according to the CDC classification [7]. Parente et al. in their multicenter study, analyzed 406 cases of OA and LA and reported a complication rate of 36.4%. Of these complications, 60.8% were Grade I and Grade II, 0.7% were Grade IIIa, 2.1% were Grade IIIb, 35.1% were Grade IVa and 1.3% were Grade V [9]. In our study, the total complication rate was 26.4%, with 18.8% of the complications classified as major (Grade IIIa and above). We believe that the lower overall and major complication rates in our study compared to the multicentric study are due to the fact that the data in our study were analyzed from a single surgeon's cases.
There are varying findings in the literature regarding the effect of BMI on the development of postoperative complications. Hauch et al. in their study examining 7829 adrenalectomy cases, identified obesity (BMI ≥ 30 kg/m2) as a significant risk factor for postoperative complications [20]. In another study examining 9820 adrenalectomy cases, a BMI of ≥ 40 kg/m2 was reported to represent a significant risk [4]. In cases where laparoscopic surgery was performed, BMI was not found to present a risk for transperitoneal procedures, but it was identified as a risk factor for retroperitoneal surgery [5, 6, 10]. In our study, due to the investigation of the E-PASS scoring system, laparoscopic (transperitoneal) and OA cases were examined as a whole, with BMI identified as an independent risk factor for postoperative complications (OR = 1.394; 95% CI = 1.158–1.677; p < 0.001).
Adhesions resulting from previous abdominal surgery can cause prolonged operative times, increased risks during the initial entry into the abdominal cavity in laparoscopic surgery, and an increase in intraoperative complications [21]. However, Morris et al. in their retrospective study of 246 LA cases found no significant difference in perioperative complication rates when comparing patients with a history of prior upper abdominal surgery to those without such a history [22]. Additionally, Mazeh et al. found that adhesions were more prevalent in cases with a history of ipsilateral and contralateral upper abdominal as well as lower abdominal surgeries. However, they observed no differences in intraoperative bleeding or the rate of conversion from LA to OA [23]. Our study also found that a history of prior abdominal surgery was not a predictor of postoperative complications. However, it should be noted that some of the LA cases we examined did involve conversion to OA.
Studies have produced varying results regarding the side of adrenalectomy and the risk of complications. In a multivariable logistic regression analysis of 462 patients, left-sided adrenalectomy was identified as an independent risk factor for postoperative complications [24]. There are also studies reporting that the side of the operation is not a risk factor for complications [25, 26]. However, the general consensus is that greater attention should be given to parenchymal and vascular structures in left adrenalectomy [3, 24]. In our study, no significant association was found between the surgical side and the risk of complications.
Adrenal surgery has been associated with a high ASA score as a significant factor in the development of postoperative complications [5, 6, 27]. Chen et al., in their study of 653 LA cases, found an increase in perioperative complications and length of hospital stay in patients with an ASA score of 3 or higher [5]. Gupta et al. examined 988 LA cases and identified that, in addition to the development of postoperative complications, the operation time was longer in the ASA 4 group [27]. The influence of performance status on surgical outcomes is well-established, with evidence showing that patients with restricted abilities in daily living activities tend to experience longer hospital stays and higher rates of morbidity and mortality [28]. However, research specifically on adrenalectomy surgery in this topic is limited [27]. In our study, it was found that, similar to existing information, a high ASA score and ECOG performance score present a risk for the development of postoperative complications (p < 0.001). Additionally, no difference in hospital stay was observed in the group with complications in our study, which is attributed to the low rate of major complications.
The Charlson Comorbidity Index is a scoring system that takes into account both the patient's age and the presence of additional chronic diseases [29]. It provides a comprehensive assessment of comorbidities, which is particularly useful in evaluating surgical risks [29]. Numerous studies have examined adrenalectomy complications using this index, highlighting its importance in predicting postoperative outcomes in patients undergoing adrenal surgery [4, 7, 30]. Although age and chronic diseases were examined in detail in our study, the Charlson Comorbidity Index was not used. Cardiac disease and diabetes were identified as significant risk factors for the development of postoperative complications (p = 002, p = 0.023 respectively). The fact that age was not found to be a risk factor for postoperative complications may be attributed to the limited number of patients > 65 years in our study.
In the literature, it has been reported that the final histopathology result of adrenalectomy generally does not affect postoperative complications [6, 10, 31]. Mellon et al. did not find statistically significant differences in the development of postoperative complications among surgeries for PHEO, CS, CuS, malignant adrenal disease and nonfunctioning adenomas [31]. Hattori et al. in their study of 265 unilateral LA cases found that the final pathology of CS, PHEO and CuS did not represent a risk for the development of postoperative complications [6]. In another study involving 610 patients, no differences were observed in the development of postoperative complications among cases with histopathology of adenoma, hyperplasia and PHEO [10]. In our study, it was observed that consistent with the literature neither the nature of the mass nor the presenting symptom represented a risk for postoperative complications. We believe that this result is due to the stabilization of patients in the preoperative period through premedication in cases of functional masses.
Large adrenal masses (> 6 cm) have been determined to be associated with increased surgical duration and a higher risk of intraoperative events during LA [5, 32]. Additionally, various studies have reported that a lesion diameter greater than 5–6 cm is an independent predictor for conversion from LA to OA [33, 34]. In our study, since OA was preferred for lesions larger than 6 cm, lesion diameter was not a significant factor in the development of postoperative complications. However, in our study, complication rates in the OA group were found to be statistically significantly higher than those in the LA group (p < 0.001). This may be due to the preference for OA in complicated cases, as well as the conversion to OA during LA in the event of intraoperative bleeding, inadequate field of view or hemodynamic instability. Additionally, the higher complication rate in patients with drain usage was thought to be related to the more frequent use of drains in OA procedures (p < 0.001).





Comments (0)