
Remember me







From January 2018 to May 2022, 785 patients underwent baseline mKRAS testing assessing plasma and/or peritoneal fluid ctDNA. Of these, 743 (95%) underwent plasma mKRAS testing, 419 (53%) underwent peritoneal mKRAS testing, and 377 (48%) underwent both plasma and peritoneal mKRAS testing. Patients in all three mKRAS testing cohorts were then followed longitudinally over the course of the study. Median follow-up was 16 months for the entire cohort.
Plasma Mutant KRAS (mKRAS) CohortOf the 743 patients who underwent baseline plasma ctDNA mKRAS testing, 639 (86%) were mKRAS-negative and 104 (14%) were mKRAS-positive. Demographics and characteristics of the two groups are seen in Table 1. The majority of patients in both cohorts were borderline resectable or locally advanced. Patients who were mKRAS-negative were more likely to have received neoadjuvant chemotherapy prior to testing compared with those who were treatment-naïve (47% vs. 16%; p < 0.001), while plasma mKRAS-positive patients were more likely to have a clinically positive laparoscopy (33% vs. 21%; p = 0.032). Overall, 227 (31%) patients underwent subsequent resection with significantly fewer mKRAS-positive patients undergoing resection (11% vs. 34%; p < 0.001). Of the resected patients, there was no difference in pathologic outcomes, including treatment response, margins, positive lymph nodes, lymphovascular invasion (LVI), or perineural invasion (PNI) between the two groups (Table 2). However, early postoperative recurrence or death within 6 months of resection was significantly more likely in plasma mKRAS-positive patients compared with mKRAS-negative patients (46% vs. 13%; p = 0.013). Overall, plasma mKRAS positivity correlated with subsequent metastatic disease (78% vs. 49%; p < 0.001) and more often hematogenous rather than peritoneal metastases (78% vs. 62%; p = 0.009). Plasma mKRAS-positive patients were also significantly less likely to be alive on follow-up (20% vs. 58%; p < 0.001). The proportion of patients who had evidence of metastatic disease or death was significantly higher in patients who were mKRAS-positive (93% vs. 62%; p < 0.001).
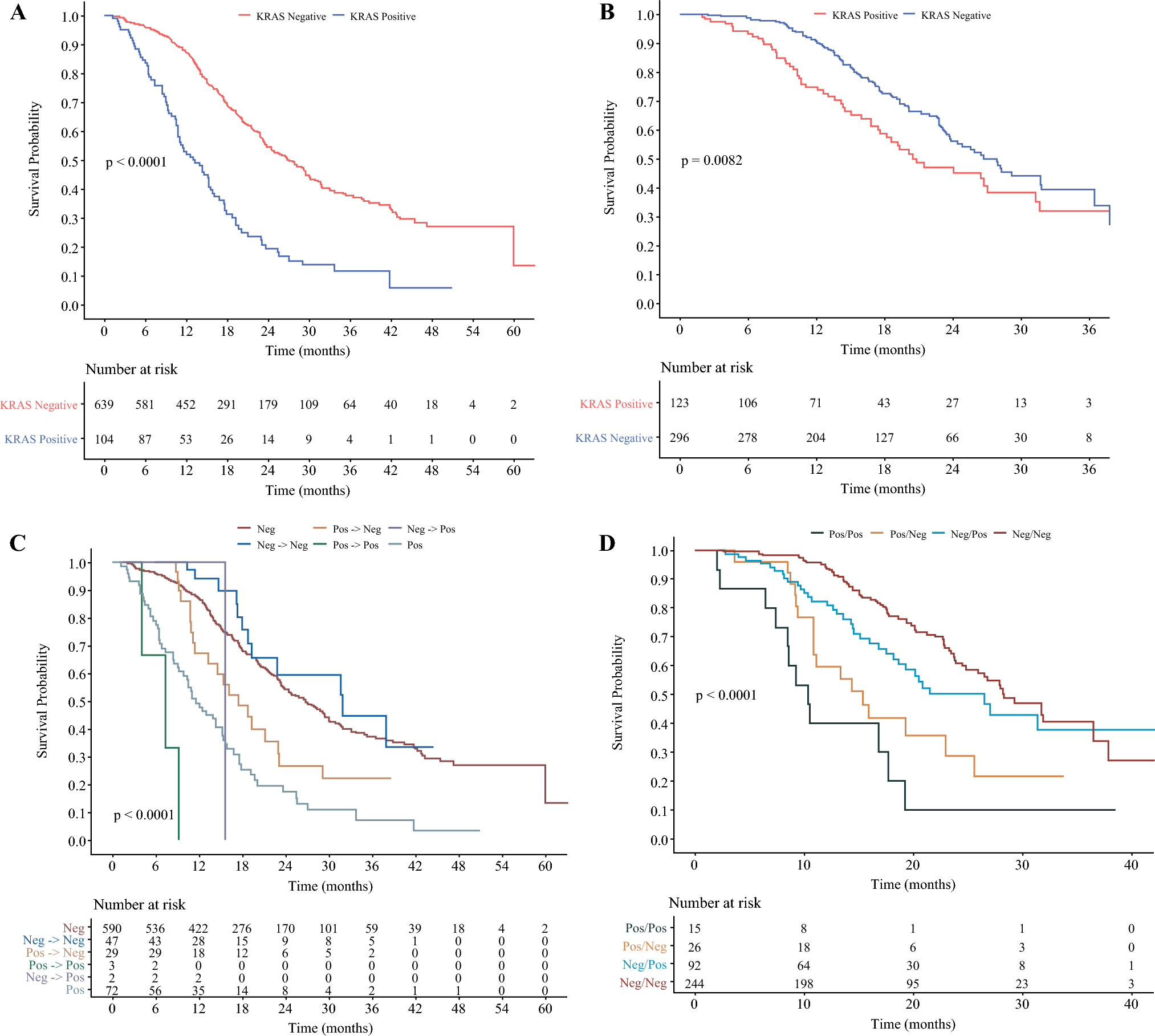
Table 1 Demographics and characteristics of all plasma and peritoneal mKRAS study patientsTable 2 Pathologic outcomes of all plasma and peritoneal mKRAS study patients who underwent resectionUnivariate survival analysis revealed significantly worse OS in patients who were plasma mKRAS-positive compared with patients who were plasma mKRAS-negative (Fig. 1a). Median OS for patients who were plasma mKRAS-positive was just 13.3 months compared with 26.9 months for patients who were plasma mKRAS-negative (p < 0.001). Additionally, positive plasma mKRAS status was a significant independent predictor for worse OS (hazard ratio [HR] 2.24; p < 0.001) on multivariable analysis (Table 3a).
Fig. 1
Unadjusted Kaplan-Meier overall survival for patients who underwent plasma KRAS testing (A), patients who underwent peritoneal KRAS testing (B), patients who underwent multiple plasma KRAS tests (C), and patients who underwent both plasma and peritoneal KRAS testing (D)
Table 3 Multivariate analysis for overall survival of plasma and peritoneal mKRAS patientsA small subgroup of patients underwent repeat plasma mKRAS testing (n = 82, 11%). Of these patients, 49 were initially mKRAS-negative and 47 (96%) of those patients remained negative on repeat testing after neoadjuvant chemotherapy. Thirty-two patients were initially positive and 29 (91%) of those patients turned negative on repeat testing after receiving neoadjuvant chemotherapy. All patients who were initially plasma mKRAS-positive and underwent resection turned mKRAS-negative with neoadjuvant chemotherapy. On survival analysis, patients who remained positive on repeat testing had a median survival of just 7 months (Fig. 1c). Patients who were initially negative but turned positive had similar overall survival (OS) to patients who were initially positive but turned negative (15.7 months vs. 17.5 months; p = 0.98), suggesting a positive plasma mKRAS at any point may be a poor prognostic factor (Table 4). Patients who remained negative on repeat testing had the best OS at 32 months. Comparisons of all plasma testing groups and survival are shown in electronic supplementary material (ESM) Table 1. In plasma mKRAS-positive patients, the quantitative plasma mKRAS copy numbers correlated with metastatic disease development and survival, with higher levels associated with death or metastatic disease (Fig. 2a).
Table 4 Comparison of overall survival between plasma mKRAS test groupsFig. 2
Quantitative plasma (A) and peritoneal (B) mKRAS results with median values noted by the horizontal line
Peritoneal mKRAS CohortOverall, 419 patients underwent baseline peritoneal fluid mKRAS testing and 123 (29%) were mKRAS-positive. Demographics and characteristics of the two groups are seen in Table 1. There was no difference in the number of patients who were concurrently plasma mKRAS-positive (p = 0.270). Peritoneal mKRAS-positive patients were much more likely to have clinically positive staging laparoscopy (53% vs. 12%; p < 0.001). Overall, 119 (28%) patients underwent subsequent resection, with peritoneal mKRAS-positive patients significantly less likely to undergo resection (21% vs. 31%; p = 0.043); however, there was no difference in pathologic outcomes between groups (Table 2). We did not find significant differences in early postoperative recurrence or death within 6 months of resection based on peritoneal mKRAS status (19% vs. 14%; p = 0.54) in contrast to resected plasma mKRAS-positive patients. Overall, peritoneal mKRAS positivity correlated with metastatic disease at follow-up (67% vs. 42%; p < 0.001) and was more likely peritoneal than hematogenous (58% vs. 26%; p = 0.009). Combined metastatic disease or death at follow-up was significantly more likely in those patients with a positive peritoneal mKRAS (76% vs. 53%; p < 0.001).
Univariate survival analysis revealed significantly worse OS in patients who were peritoneal mKRAS-positive (Fig. 1b). Median OS was 20.8 months for the peritoneal mKRAS-positive patients compared with 27.9 months for the peritoneal mKRAS-negative patients (p = 0.008). On multivariable analysis, peritoneal mKRAS positivity was an independent predictor of worse OS (HR 1.46; p = 0.025) (Table 3b). Similar to the plasma mKRAS cohort, quantitative peritoneal mKRAS copy numbers detected correlated with metastases and survival, with higher levels associated with death or metastatic disease (Fig. 2b).
Combined Plasma and Peritoneal mKRAS CohortOverall, 377 patients underwent both baseline plasma and peritoneal mKRAS testing concurrently as they were enrolled in both prospective studies. For analysis, these patients were organized into four groups based on compartment-specific mKRAS status: positive plasma and peritoneal mKRAS (Pos/Pos); positive plasma mKRAS and negative peritoneal mKRAS (Pos/Neg); negative plasma mKRAS and positive peritoneal mKRAS (Neg/Pos); or negative plasma and peritoneal mKRAS (Neg/Neg). The majority of patients were Neg/Neg (n = 244, 65%), with just 4% (n = 15) being Pos/Pos.
On univariable survival analysis, patients who were Pos/Pos had the worst survival, with a median OS of just 10.4 months (Fig. 1d). Patients who were Pos/Neg had a median OS of 15.4 months and Neg/Pos patients had a median OS of 26.5 months. Patients who were Neg/Neg had the longest median OS of 28.4 months (p < 0.001). Any positive mKRAS test regardless of compartment was associated with worse outcomes (Table 5a). Furthermore, the presence and location of metastases varied on the compartment-specific mKRAS status. Patients with a positive plasma mKRAS were more likely to develop hematogenous metastases (56% vs. 27%; p < 0.001) and those with a positive peritoneal mKRAS were more likely to develop peritoneal metastases (40% vs. 11%; p < 0.001) [Table 5b]. In the Pos/Pos group, 93% of patients developed metastases or had died at last follow-up compared with only 50% in the Neg/Neg group (p < 0.001) (Table 5b).
Table 5 Combined mKRAS compartment status for (a) overall survival and (b) metastases or death, type of metastases, and mKRAS copy numberOn multivariable analysis, mKRAS status was a significant predictor of worse OS, with increasing survival hazard based on compartment-specific mKRAS status (Table 3c), with worse outcomes in the Pos/Pos group (HR 4.02; p < 0.001).
Finally, we assessed the diagnostic accuracy of both plasma and peritoneal mKRAS compared with plasma and peritoneal tumor markers to predict metastases and death (ESM Table 2). Plasma mKRAS positivity was less sensitive than plasma CA19-9 levels but was significantly more specific. Peritoneal mKRAS positivity had similar low sensitivity but high specificity comparable with peritoneal fluid CA19-9 and CEA levels.
Comments (0)