
Remember me





This prospective randomized single-center study was conducted in adherence to the CONSORT guidelines.
Study populationEligible patients who met the inclusion criteria and scheduled for surgical treatment due to benign prostatic obstruction (BPO) caused by benign prostatic hyperplasia (BPH). The study was approved by the ethical committee (ZU-IRB No. 9938). Written informed consent was obtained from all patients, and the study period was from October 2022 to March 2024.
Inclusion criteriaPatients with BPH and prostate size between 40 and 80 g as measured by transrectal ultrasound (TRUS), An International Prostate Symptom Score (IPSS) greater than 20, A maximum urinary flow rate (Qmax) of less than 10 ml/s. Sexually active individuals with a normal marital life with International Index of Erectile Function-5 (IIEF-5) score more than 22.
Exclusion criteriaPatients with systemic disease, diabetes mellitus, or neurological disorder having an impact on antegrade ejaculation. Patients with bladder or urethral pathology.
Sample sizeAssuming an overall satisfaction score of 6 ± 2.4 for the Ejaculatory Hood Spring compared to 4 ± 2.1 for the standard group [12], with a power of 80% and a 95% confidence interval, and accounting for a 10% dropout rate during follow-up, the estimated sample size was 40 cases, with 20 cases in each group. (Open Epi, Version 3.01). This study was designed to detect the rate of retrograde ejaculation (RE) as the primary outcome and evaluate the urinary incontinence (UI) rate as the secondary outcome.
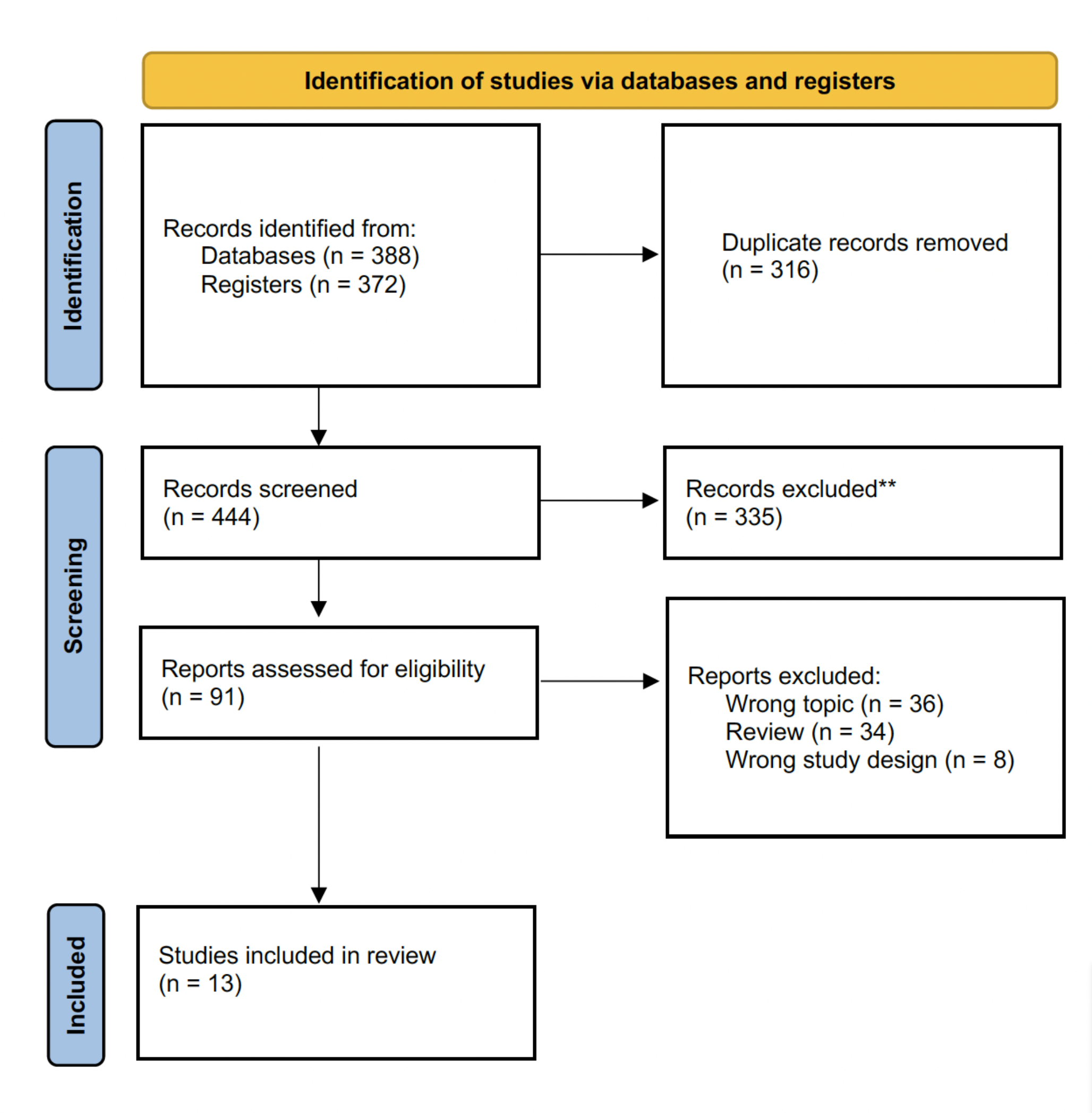
RandomizationPatients were randomized using a computer-generated allocation sequence. A total of 48 patients were assessed for eligibility, and ultimately, 43 patients were randomly assigned in a 1:1 ratio to receive HoLEP or EP HoLEP.
Outcome measuresThe primary endpoints of the study included early postoperative continence assessment at 1- and 3-month, measured by the International Consultation on Incontinence Questionnaire-Urinary Incontinence Short Form (ICIQ-UI SF) in both groups. Secondary endpoints included changes in Male Sexual Health Questionnaire-Ejaculatory Dysfunction Short Form (MSHQ-EjD-SF) scores from baseline to postoperative, IIEF-5, and the assessment of lower urinary tract symptoms (LUTS) relief using IPSS, Qmax, and quality of life (QoL). Perioperative adverse events were also compared and reported. We defined postoperative UI as reported by a patient (stress UI, urge UI, and dribbling after urination).
Perioperative workupThe baseline workup included a clinical examination, digital rectal examination. Laboratory and radiological evaluations consisted of serum prostate-specific antigen (PSA), pelvic-abdominal ultrasound, prostate volume measurement by (TRUS), and uroflowmetry. All patients were assessed using the IPSS, Qmax, QoL, IIEF-5, and MSHQ-EjD-SF both preoperatively and postoperatively.
Description of equipment and surgical techniqueA 26F Storz continuous flow resectoscope with separate laser bridge and 0.9% saline was utilized. The laser equipment used included 550 μm fiber and a 100W holmium-YAG machine (Sphinx® LISA Laser Machine, Germany), set to a power of 1.5–2 J at 40–50 Hz. Resection of the enucleated prostatic adenoma was performed using a Storz standard bipolar cutting loop, followed by retrieval of residual tissue with an Ellik evacuator. At the end of the surgery, a 22-F three-way catheter was inserted and retained until the urine was clear.
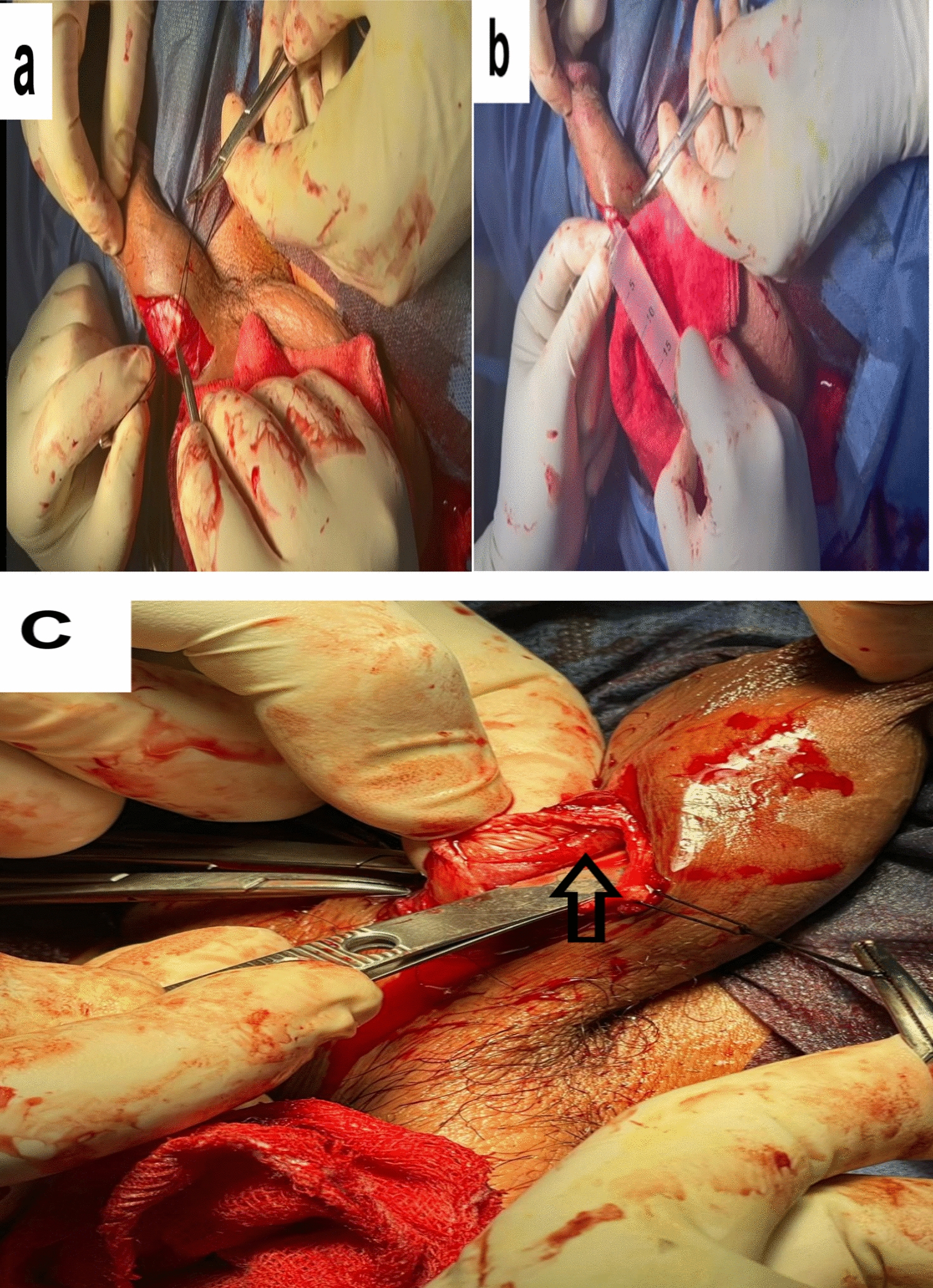
Surgical techniqueTwo experienced surgeons performed the procedures, each having completed over 180 HoLEP surgeries. All patients received prophylactic intravenous antibiotics 60 min prior to surgery, which was conducted under spinal anesthesia. In Group 1, the standard HoLEP enucleation was performed as outlined by Gilling [1]. In Group 2, we conducted Ejaculatory Preservation (EP) HoLEP by implementing a preservation maneuver during the trilobar gland enucleation of the median lobe. This involved leaving approximately 10mm proximal to the verumontanum and 5mm paracollicular of the lateral lobes intact (Fig. 1a). Additionally, 5mm of mucosal attachments to the bladder neck were preserved by trimming the bladder neck at the 5 and 7 o’clock positions (Fig. 1b). At the 2 o’clock and 10 o’clock positions, we spared the mucosal strip extending from the bladder neck at the 12 o’clock position down to the urethral lumen at the level of the verumontanum (Fig. 1c). For the bilobar gland, the incision was made at the bladder neck at the 5 and 7 o’clock positions and extended distally along the capsular plane to 10mm proximal to the verumontanum. An intact mucosal strip was maintained from the bladder neck at the 6 o’clock position to the verumontanum. The lateral lobes were enucleated using the same technique applied to the trilobar gland.
Fig. 1
Illustrates the ejaculation preservation technique. a Identify the prostate's anatomical region (Tri/Bilobar) and create incisions at 5 and 7 o'clock, joining them 10 mm above the veru. b Completely dissect the middle lobe, leaving it attached at the bladder neck. c Preserve the mucosal strip at 2 and 10 o’clock, extending from the bladder neck (12 o'clock) till the level of the veru. d Spare the mucosal strip at 2 and 10 o'clock, connecting at 12 o'clock, Strike*. e Preserve mucosal attachments to the bladder neck from the middle lobe at 5 and 7 o'clock, Strike*
Postoperative follow-upPatients were scheduled for follow-up at 1-, 3-, and 6-month post-surgery. Outcome measured were ICIQ-UI SF, IPSS, Qmax, QoL, IIEF-5, and MSHQ-EjD-SF. Delayed complications were addressed. Patients were also advised to resume sexual activity after catheter removal.
Statistical analysisStatistical analysis was conducted using SPSS V23.0 (IBM Corp, Armonk, NY). Parametric data were analyzed with an unpaired Student’s t-test, categorical data with the Chi-square or Fisher's exact test, and nonparametric data, presented as median and range, with the Mann–Whitney test. The significance level was set at P < 0.05.
Comments (0)