We present progression and survival data from a multi-institutional cohort of patients with ependymoma treated with a range of radiotherapy doses. We also assess factors associated with disease progression and examine characteristics of a subgroup of patients with relapse after radiation. While our findings support the use of radiotherapy doses ≥ 59.4 Gy in the management of intracranial ependymoma, they also point to underlying biological factors such as age as important drivers of survival after treatment.
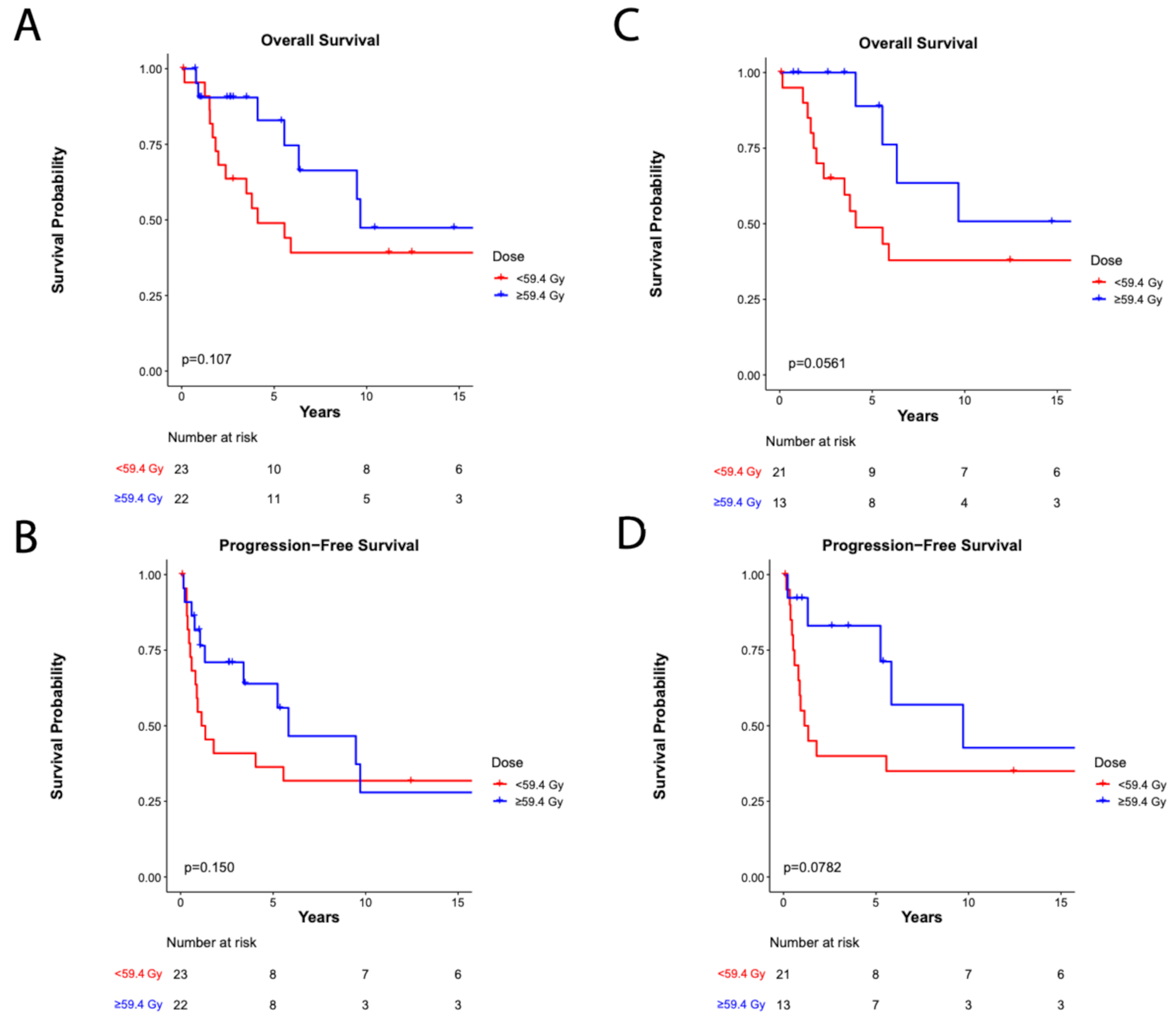
Doses ≥ 59.4 Gy were not associated with better OS or PFS in the cohort as a whole; however, we found a trend towards improved outcomes among patients with grade 2 ependymoma treated with higher doses. While no randomized studies have compared radiation dosing regimens in this patient population, a large, prospective study including 131 patients treated to 59.4 Gy demonstrated excellent seven-year event-free survival and OS rates of 69.1% and 81%, respectively [3]. These findings confirmed the safety and feasibility of dose-escalated radiotherapy in the upfront setting for patients ≥ 18 months old. More recently, a trial conducted by the Associazione Italiana di Ematologia e Oncologia Pediatrica (AEIOP) found higher rates of five-year PFS and OS among patients who received an 8 Gy boost to residual disease compared with historical controls [14], supporting the use of high-dose radiation in a patient subgroup with consistently poor outcomes [2]. Several retrospective studies have since examined the impact of dose on survival with varying results. A National Cancer Center Database analysis of patients > 2 years old who received 54 Gy versus ≥ 59.4 Gy failed to show a difference in OS between dose groups [15]. Of note, the median age of patients in this study was 24, significantly higher than the median ages of 2.6 and 9.1 years in the < 59.4 Gy and ≥ 59.4 Gy groups in our cohort. Adolescents and young adults tend to have better outcomes compared with younger children [16] and may therefore benefit less from dose-escalated treatment. This is consistent with results from Ager et al., who found that doses > 54 Gy correlated with improved OS in patients ages 2 to 18 but not in those over 18 [17].
Within the last decade, molecular profiling has led to the discovery of nine distinct ependymoma subgroups [18] that have since replaced classical histopathologic grading in the 2021 WHO classification scheme [19]. These subtypes correlate closely with features such as age of presentation and disease location (i.e., supratentorial versus infratentorial). For example, both the PFA and PFB subtypes are characterized by posterior fossa tumors; however, PFA ependymomas occur primarily in infants and young children while PFB tumors are more often found in adolescents and young adults [20]. Importantly, the PFA subtype has been associated with worse outcomes [18]. This may explain our finding of shorter PFS among patients ≤ 4 years old at diagnosis, although we unfortunately did not have molecular subtyping available for patients in this cohort. Of note, considerable heterogeneity exists within each PF subtype [21, 22] and the prognostic implications of these molecular features remain controversial, with ACNS0121 [2] failing to detect a difference in PFS, OS, or failure pattern between PFA and PFB tumors. Larger studies of more modern ependymoma cohorts with molecular subtyping are needed to further understand the relationship between age and survival.
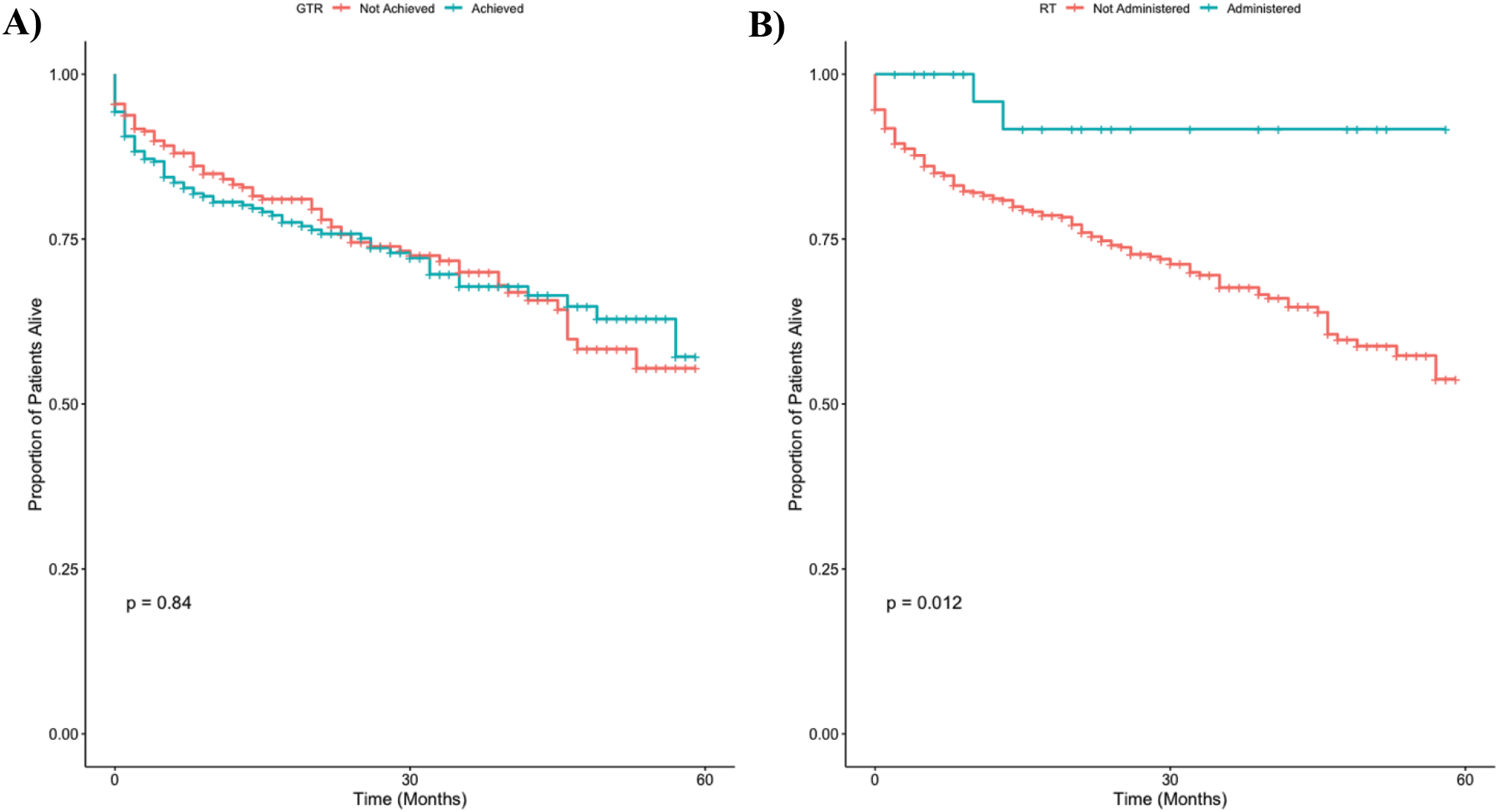
Notably, STR, which has consistently been linked to poor oncologic outcomes and survival, did not portend an increased risk of progression in this cohort. While the risk of progression up to five years after radiation was clearly higher among patients who underwent STR (Supplemental Figure S1), there were multiple late recurrences in the GTR group that ultimately obscured any early PFS advantage in these patients. The relative infrequency of patients with STR in this study (20.0%, versus 80.0% with GTR) likely also contributed to a non-significant difference in PFS between these groups. Another possible explanation for this finding may be related to underlying imbalances in the distribution of ependymoma subtypes between patients who underwent GTR versus STR. Indeed, these subgroups enhance patient risk stratification compared with other traditional clinical risk factors such as extent of resection [23] and tumor location [20]. Further investigation into how these novel molecular subgroups will influence classic treatment paradigms is needed.
We also describe the clinical features, management, and outcomes among a subset of 24 patients who ultimately relapsed after upfront radiotherapy. The median time to relapse was 0.8 years, consistent with prior studies of recurrent ependymoma [13]. Relapse times among patients in our cohort ranged from 0.2 to 9.7 years, reflecting the potential for a long latency period between initial treatment and disease recurrence that is characteristic of ependymoma [10]. Consistent with prior literature [5], most patients had progression of disease within the original radiation field. Management upon disease recurrence varied. As shown in prior studies [13], salvage surgery (61% of patients) and reirradiation (48%) were the most commonly used treatment modalities at progression. Optimal management at the time of relapse is unknown. Prior studies have shown favorable outcomes among patients who undergo salvage surgery, specifically among those who achieve a GTR [10, 24]. Re-irradiation has also demonstrated efficacy upon recurrence, with three-year OS rates ranging from 48–81% [25,26,27,28]. Various radiation modalities have been explored in the relapse setting, including conventionally or hypofractionated focal radiation [24], stereotactic radiosurgery [29], and craniospinal irradiation (CSI) [30, 31]. The role of salvage chemotherapy remains controversial. A wide range of regimens are currently used [24], and it is typically recommended when surgery and radiotherapy are not feasible [32]. Indeed, patients in this cohort and others [10, 24, 33] who received salvage systemic therapy had worse survival, likely due to selection bias for patients unable to get local therapy or those with more widespread disease. The lack of survival advantage seen with surgery, radiation, or chemotherapy in this study reflects the complexity of management of recurrent ependymoma. More robust exploration of optimal treatment strategies at the time of relapse are needed, particularly given that about one-third of patients ultimately recur [34].
Rates of brainstem necrosis, a rare but devastating potential complication of ependymoma treatment, were low in this cohort. This is consistent with prior studies examining the risk of brainstem necrosis after photon radiotherapy to the posterior fossa [35, 36]. One patient developed grade 3 brainstem necrosis after undergoing reirradiation with protons, both of which have been identified as risk factors for brainstem toxicity [37, 38]. Fortunately, modified consensus treatment planning guidelines and revised proton-specific brainstem constraints continue to improve the safety profile of posterior fossa radiation [36].
This study has several limitations, many of which are related to its retrospective nature. We were unable to avoid selection bias towards treating patients with more aggressive disease with higher radiation doses; patients with grade 3 ependymoma and those who received post-radiation chemotherapy were more likely to be treated to ≥ 59.4 Gy. Nevertheless, we also specifically examined the association between radiation dose and survival in patients with grade 2 disease, where there was a trend towards improved OS and PFS with higher radiation doses. Our sample size was relatively small; therefore, comparisons of outcomes between various patient subgroups may have been underpowered. In addition, given the small sample size, we were unable to perform other types of analyses, including propensity score matching. Notably, few patients underwent STR, which may have contributed to our lack of finding a link between extent of resection and risk of progression. Nevertheless, we had long follow-up from patients treated at multiple institutions, including 24 patients with relapsed disease. There was no central review of baseline pathology and imaging, which may have altered the baseline characteristics of patients in our cohort, including assigned histologic grade [39]. Finally, we did not have information on molecular tumor subtypes for these patients and were therefore unable to determine whether subgroups were balanced between the < 59.4 Gy and ≥ 59.4 Gy cohorts. Notably, patients receiving < 59.4 Gy were significantly younger; therefore, it is possible that these patients demonstrated earlier progression due to underlying biological differences in their disease (i.e., higher likelihood of PFA subtype) rather than suboptimal radiation dosing. This may also explain why traditional risk factors such as upfront extent of resection did not appear to influence survival in this study. It is unclear if our findings would have changed had these subgroups been considered.
In conclusion, we present the characteristics, management, and outcomes from a multi-institutional cohort of patients with intracranial ependymoma treated with radiotherapy. Our findings suggest that higher radiation doses may improve outcomes in patients with grade 2 disease and confirm the poor prognostic significance of younger age. Further research into the management of relapsed ependymoma is needed. Optimal radiation dosing remains unknown in the era of molecular subtyping. Prospective trials that describe outcomes among molecular subgroups such as COG ACNS0121 [2] and ACNS0831 [11] may provide better insight into which patients benefit most from higher doses.






Comments (0)