
Remember me

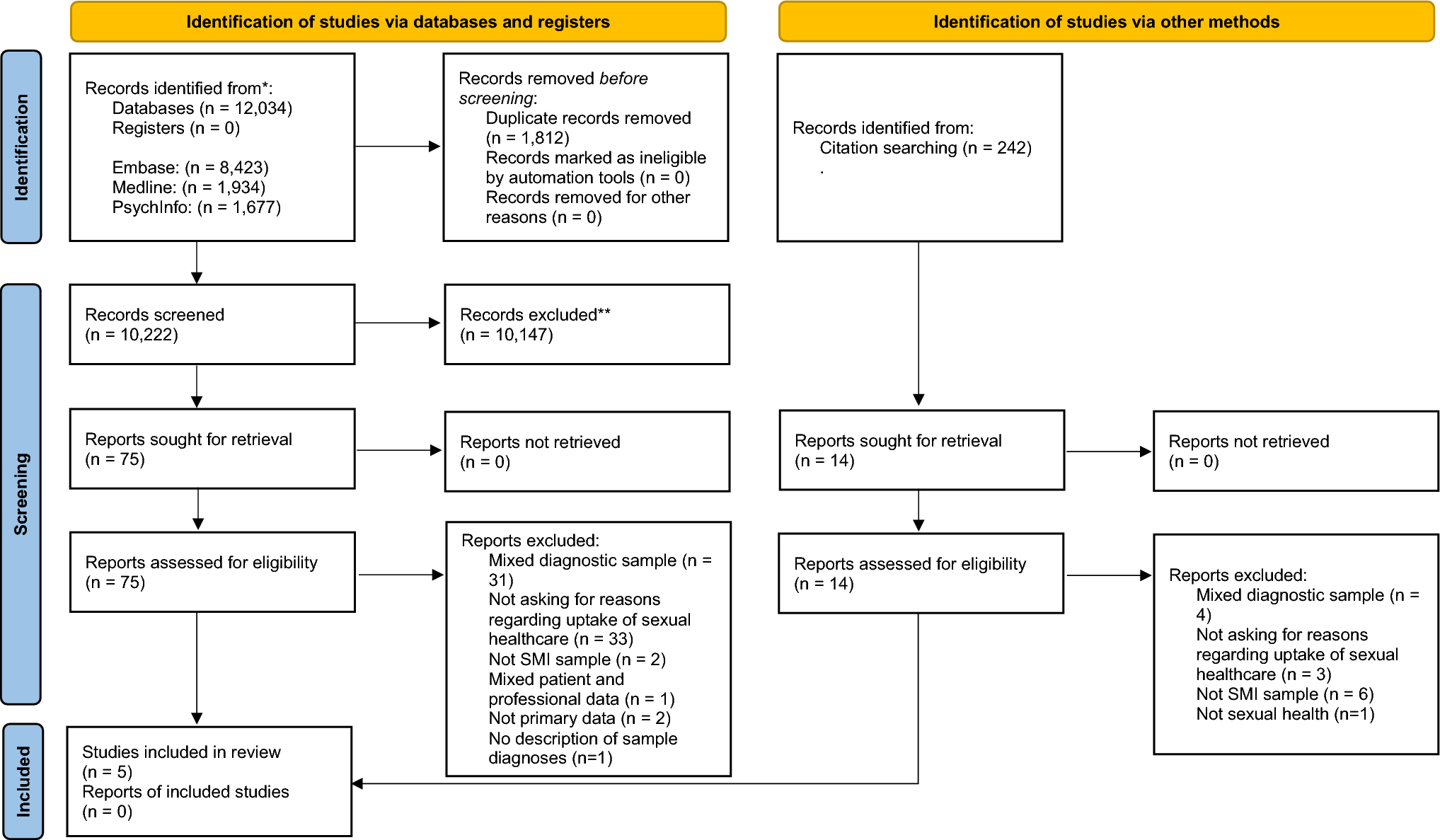
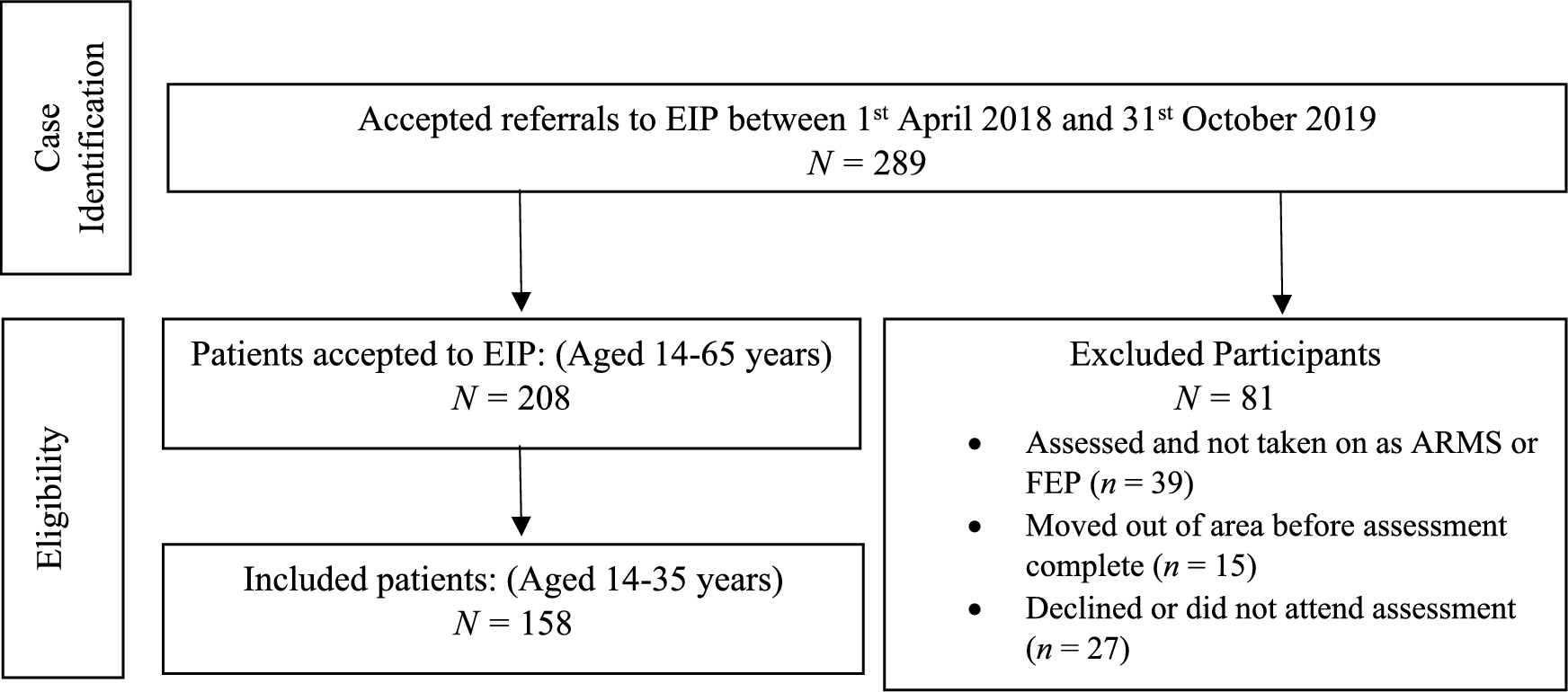

The total number of papers identified was 12,034. After removing duplicates, 10,222 unique references were eligible for title and abstract screening. Of these, 10,147 were excluded, leaving 75 to be examined by full text. Five studies were deemed appropriate for inclusion in this review [25,26,27,28,29]. Reasons for excluding 70 full texts are presented in the PRISMA flowchart in Fig. 1.
Fig. 1 Study characteristics
Study characteristicsThe key characteristics and quality appraisal scores of the included studies are reported in Table 1. In one case [26], the geographical location of the research was not stated, thus, it was assumed based on the author’s backgrounds. There was no other missing information across the papers. Publication dates ranged between 1998 and 2024. Three were from studies based in the US, one in Canada, and one in South India. Three studies had female-only samples, whilst the other two were majority male. Two focussed on HIV care, two on family planning, and one focussed on general sexual and reproductive healthcare. One study solely focussed on schizophrenia and one included people with psychosis more generally, whilst the others also included diagnoses of bipolar disorder, schizoaffective disorder, and major depression with psychotic features.
Table 1 Key characteristics of the five studies included for reviewMethodological qualityThe quality assessment (Table 1) indicated that two studies had a high quality [25, 29], and three had a medium to low quality [26,27,28]. The studies were mostly limited in their measures of barriers and facilitators to accessing sexual health care, as well as their identification and handling of confounding variables.
Barriers to accessing sexual healthcareThe results have been grouped by the type of sexual health service each study assessed: access to HIV services; access to family planning methods; and access to general sexual healthcare.
Access to HIV careTwo studies investigated access to HIV care [25, 28], both US-based and included a range of diagnoses under SMI. Diagnoses were gathered from medical records and agencies. Their samples were majority male and ranged from 18 to 50 years old.
Fremont et al. [25] adopted a structured interview approach to examine experiences of HIV care for people with SMI versus those without. Their main study outcomes compared HIV care between groups based on residency in Los Angeles or New York City, considering barriers to HIV care as a secondary outcome. The two questions asked about barriers to care regarded needing physical healthcare but being unable to “get it” and going without health care due to cost of living issues (See Table 1). They reported that people with SMI are less likely to obtain and more likely to decline HIV care due to cost compared to people with HIV and no SMI but did not report exact figures for each group.
Considering risk of bias assessment, Fremont et al. [25] scored 8/10 (80%), mostly due to sound matching of cases and controls, measurements of exposure, and handling of confounding variables. However, their assessment of barriers to HIV care remains questionable. The authors measured barriers to HIV care with two single items from the national HIV Cost and Services Utilisation Study (HCSUS) [25]. These were pre-defined to ask about cost, one item not being mentioned until their discussion. Adaptations of these items were not evidenced as validated, and the authors failed to mention any reliability check of participant responses, therefore hindering the internal validity and inter-rater soundness of their findings.
Sullivan et al. [28] undertook a cross-sectional study concerning the difference in utilisation and satisfaction of healthcare when receiving HIV and mental health support at single or separate sites, comparing SMI to non-SMI groups. They assessed hospital experiences, communication between separate sites, and barriers to obtaining care. Like Fremont et al. [25], their assessment of barriers to HIV care was taken from the HCSUS survey, using a three-item index of closed questions concerning the proportion of participants who believed they could not obtain care due to insufficient funds and other priorities. They found that some participants with SMI reported experiencing cost as a barrier to HIV care (17%). On the one hand, these findings can be perceived as positive outcomes, yet their sample involved clients who had already gained access to services, and these findings must be considered in the context of the risk of bias.
A score of 5/8 (62.5%) was given to Sullivan et al. [28], representing mid-quality evidence. Their handling of confounding variables and method of measuring communication between HIV and mental healthcare sites was unclear. Additionally, although their closed questions on barriers to HIV care indicated yes/no responses, the proportion of agreement on each item, for example, not accessing care due to lack of money versus needing food, are omitted. Thus, findings remain somewhat limited.
Access to family planning methodsThe oldest and most recent studies focussed on family planning practices for women with SMI [26, 27], both adopting semi-structured interview designs. Whereas Miller and Finnerty [26] included a range of diagnoses assessed by the RDC [21], Sethuraman et al. [27] only included women with an ICD-10 [19] diagnosis of schizophrenia. Both reported similar age ranges of participants (See Table 1).
Miller and Finnerty [26] compared women with and without SMI. They gathered data on sexuality and reproductive experiences, including attitudes and practices of birth control methods. Their interview schedule took instruments from previous work, creating a “Family Planning Interview”. After receiving spontaneous responses from women with SMI about why they were not using contraception, the researchers provided participants with 16 pre-defined reasons, asking women to indicate which applied to them. Reasons that were statistically more common in women with SMI than those without were “Didn’t get around to it” at 31% versus 12%, and “Too hard to get birth control” at 25% versus 0%. In relation to birth control being hard to get, the authors do not report any exploration of this item. “Birth control doesn’t work” was also higher at 15% versus 2% but not statistically different between the groups. The most common reason among those with SMI were “Didn’t expect to have sex” (46.5%) and not “Didn’t think about birth control or pregnancy while having sex” (45.2%). All reasons reported can be found in Table 1.
In terms of quality assessment, the interviewers in Miller and Finnerty’s [26] study were trained by professionals, and the responses of women with SMI were checked with clinicians, boosting the reliability of their findings. However, Miller and Finnerty [26] failed to cite where the 16 coded answers were derived from, and did not report the details of the qualitative accounts from their participants. Therefore, potentially core information on barriers to contraception use was omitted. Consequently, some risk of bias is introduced when deeming these results from the perspectives of women with SMI. Their study scored 6/10 (60%) on the risk of bias assessment, representing mid-quality evidence.
Whilst the previous papers were all US-based, Sethuraman et al. [27] examined birth control attitudes and practices among women with SMI in South India. Their interview protocol was adapted from the National Family Health Survey (NFHS-3 [30]), however, Sethuraman et al. [27] do not explicitly state whether the question on reasons for not using contraception elicited open-ended or closed responses. Around a third of participants were not using contraception at the time of data collection, and almost 15% had unmet contraceptive needs. Wanting to become pregnant (45.2%), lack of awareness (35.5%), and not receiving information about family planning from mental health services (32.3%) were the most frequently reported reasons for not using contraception.
Sethuraman et al. [27] scored 4/8 (50%) on the risk of bias assessment, indicating relatively poor quality of evidence. Whilst they failed to indicate whether they collected spontaneous responses from participants, semi-structured interviews are an exploratory tool usually involving qualitative data gathering [31]. As such, open-ended answers likely to be rich in validity appear to be missing in this report. Furthermore, one author collected and presumably interpreted their data, yet the process and reliability of evidence synthesis remains ambiguous.
Access to general sexual healthcareOne study by Barker et al. [29] investigated access to general sexual healthcare. This was with women (cisgender, transgender and nonbinary/gender-diverse women) with psychosis in Canada. It included information from both service users and clinicians, although the latter is not discussed here. This was a qualitative study based on semi-structured interviews. Although the focus was experiences of sexual and reproductive healthcare access and utilisation, this naturally raised issues around barriers and facilitators to care.
Several barriers to care were highlighted. Psychotic symptoms, particularly paranoia and disorganisation, hindered service users’ ability to trust professionals, arrange appointments, and engage in care offered. While not explicitly described as a barrier, some service users reported prioritizing mental health care above other health needs, which can lead to neglect of sexual health concerns.
Mental health stigma was raised as an issue by participants, especially in relation to decisions to have children, and the discomfort around discussing sex. Service users described a lack of attention to sexual and reproductive health in mental health programmes and struggled to initiate conversations about sexual health. When issues were raised, participants reported solutions were not always provided by their care providers.
A lack of sexual health knowledge was also noted. Some respondents turned to physicians for advice, while others reported using the internet and media for information. Culture, religion, and ethnicity were raised by multiple service users as barriers to access care. Financial barriers, particularly in relation to contraception, were also raised.
Finally, service users described challenges in accessing specialized services for sexual difficulties like dyspareunia, but the paper did not provide detailed descriptions of these challenges. The study received a risk of bias score of 10/10.
Facilitators to accessing sexual health servicesOnly Barker et al. [29] reported on facilitators to accessing sexual health services for people with SMI. As discussed above, barriers and facilitators were not the focus of this paper, however, in the process of exploring experiences of sexual and reproductive healthcare, some facilitators were highlighted. Service users discussed how siloed mental health and sexual health services allowed a degree of anonymity that made it easier for them to access care. This was the only facilitator discussed.
Comments (0)