Study design
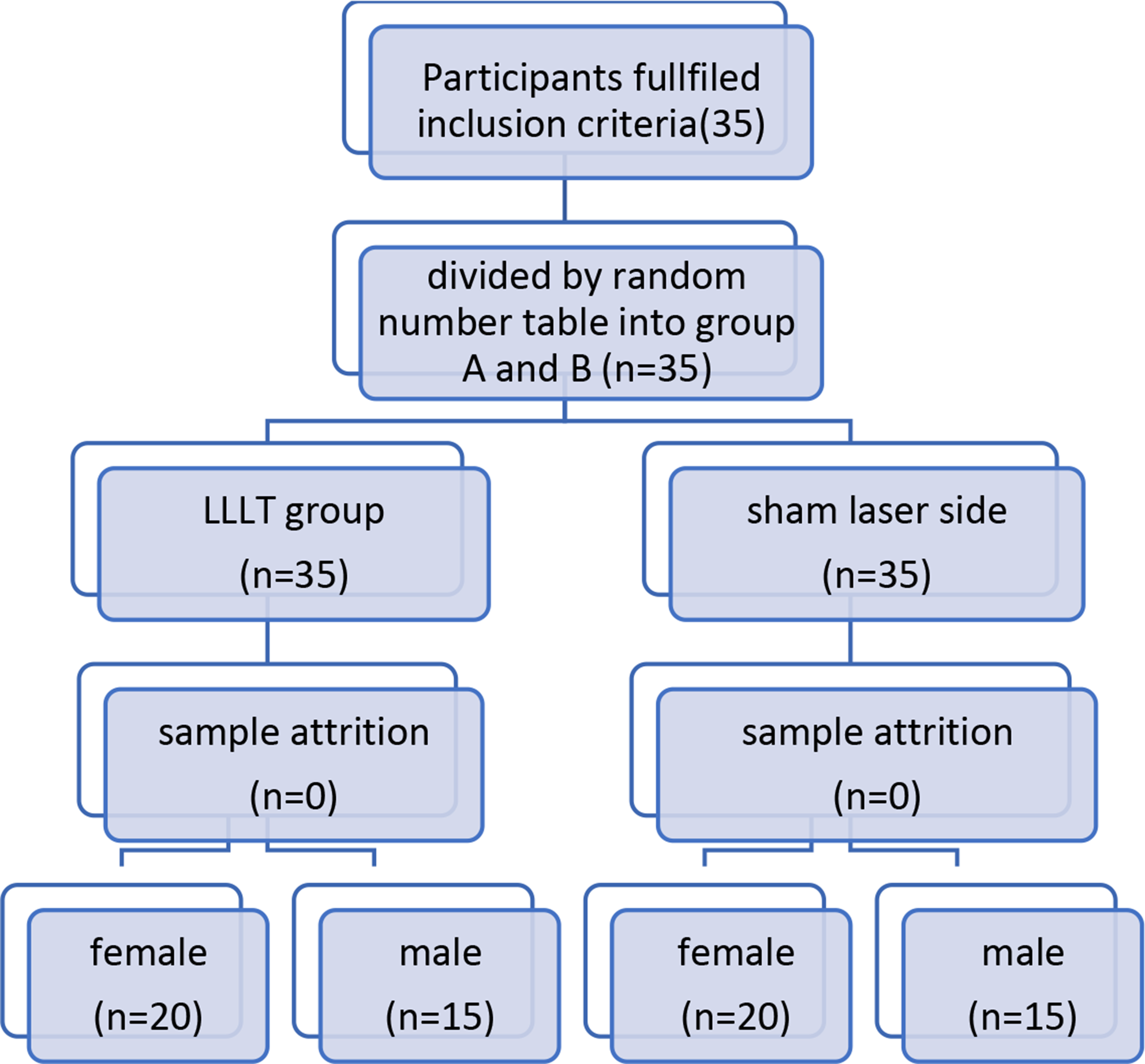
This study was designed as a comparative, prospective study. It was approved by the local ethics committee (2022–100893-BO-ff; 2023–101110-BO-ff), preregistered in clinicaltrials.gov (NCT06431282), and applied in accordance with the Good Clinical Practice and Declaration of Helsinki. Healthy female and male subjects were recruited. Exclusion criteria were pregnancy, breast feeding, open wounds or lesions at the area to be treated. After informed consent, subjects were assigned to a laser treatment using a fractional 10,600 nm CO2 laser or a fractional 1927 nm Tm laser with and without subsequent application of a weakly-crossed HA preparation. Subjects were measured 30 min (visit V1) and followed-up 30 days (visit V2) after treatment using an MPT-FLIM system. Data on the CO2 laser treatment group were published previously [4].
Treatment protocol
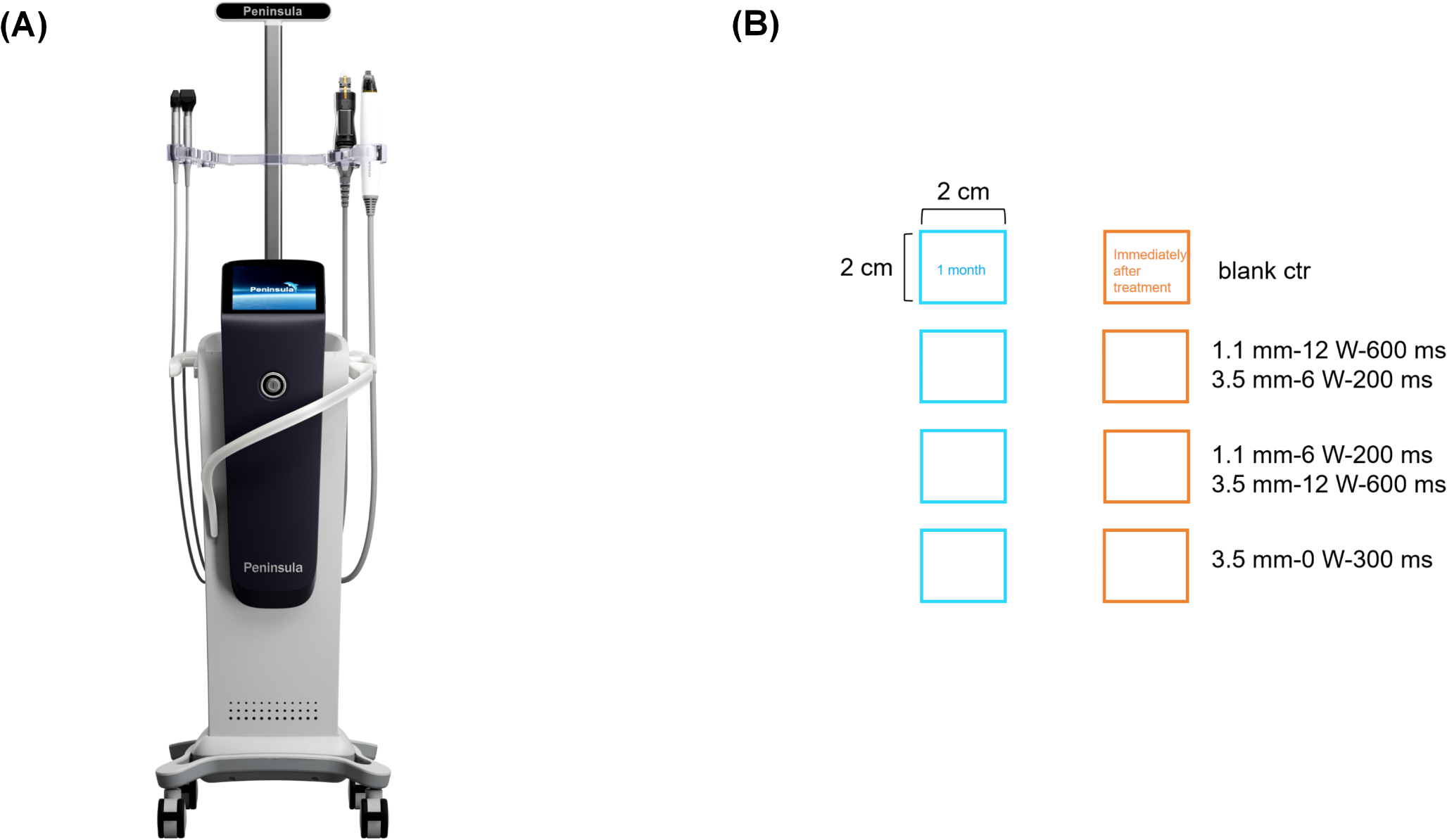
For each volunteer, four squares were marked on the right or left forearm: (i) laser with subsequent SQB application, (ii) laser monotherapy, (iii) SQB application monotherapy, and (iv) untreated control. The squares were marked on a transparent foil to ensure consistency in follow-up measurements.
Prior to the CO2 laser treatment (eCO2 Plus™, Lutronic Medical Systems, Hamburg, Germany), participants received a local anesthetic ointment (23% lidocaine, 3.5% tetracaine, 3.5% tetracaine-HCl) under occlusion on the area to be treated for 30 min. After thorough cleansing and disinfection, participants were treated with the following parameters: 120 µm, 40 mJ, 30 W, 8 mm square, 5.8% density. For the Tm laser treatment (LaseMD UltraTM, Lutronic Medical Systems, Hamburg, Germany), following parameters were applied: C1 handpiece, random mode, 5 mJ, 6 passes. Here, local anesthesia was not necessary.
Directly after laser treatment, 0.5 ml of an SQB (Restylane Vital light® Skinboosters™, Galderma®, Lausanne, Switzerland) was applied on the marked squares under occlusion for 30 min. Participants were advised to avoid extensive UV exposure or HA-containing topicals on the treated areas for 30 days post-treatment.
Multiphoton tomography with fluorescence lifetime imaging
A CE-certified MPT-FLIM system (MPTflex, JenLab GmbH, Berlin, Germany) was applied. We used a titanium:sapphire tunable laser system (Mai Tai, Newport Spectra-Physics, Santa Clara, CA, USA) to provide near-infrared laser pulses for excitation of endogenous fluorophores and inducing SHG. The technical setup consisted of a Glan calcite polarizer, two galvanometric mirrors, a beam expander, and a collimator. Laser pulses were reflected into a 40 × oil immersion objective with a numerical aperture of 1.3 (Carl Zeiss Jena GmbH, Jena, Germany). Photomultipliers (PMT) combined with time-correlated single-photon counting (TCSPC) were used for image acquisition.
Data acquisition
Biogenic fluorophores and SQB were excited at a wavelength of 760 nm. For each region of interest, two or three z-stacks of 100 µm × 100 µm images were acquired from the corneal to the dermal layer up to a depth of around 150 µm with 1.5 µm increments. We performed time-correlated single photon counting (TCSPC) using a TCSPC module (SPC 830, Becker & Hickl GmbH, Berlin, Germany) and analyzed the resulting data using SPCImage 8 software (SPCM, Becker&Hickl GmbH, Berlin, Germany). Mean fluorescence lifetimes (τm) were calculated to objectively assess the inflammatory cellular state and was defined as [10, 12]:
τ1 represents the lifetime of free NADH, while τ2 corresponds to the lifetime of protein-bound NADH, with a1 and a2 denoting their ratios. The data was then pseudo-colored (from 100 ps (red) to 2,000 ps (blue) for illustrative purposes.
Statistical analysis
We performed the statistical analysis using GraphPad Prism (Version 9, Graphpad Software, Boston, USA). Descriptive data are presented as means ± standard deviation and ranges (minimum – maximum). The paired t-test was used to determine the difference in mean between groups unless stated otherwise. P-values < 0.05 were considered significant.






Comments (0)