The explicit framing of health as a security issue is often linked to the early 2000s —conflated by 9/11- when the UN Security Council adopted resolution 1308, portraying HIV/AIDS as a security issue motivated by the inherent concern around combat effectiveness. [14, 32]. Ethical implications of framing HIV/AIDS as a matter of security have been challenged and explored [15, 18]. Nonetheless, such framing has produced policy responses for the protection of high-income individuals, groups, or nations, as evidenced by a focus predominantly overseas [30, 32, 33]. While this does not negate that the funding and resources it has leveraged have benefited recipient countries, it does raise a critical question: when—or why—is it not enough to simply call a health issue that requires attention, even urgent attention, a public health issue? Might there be a moral dilemma in pursuing a security-charged agenda?
The United States Centre for Disease Control and Prevention (CDC) defines health security as a state of resilience specifically to infectious disease threats; i.e., health security as “resilient public health systems that can prevent, detect, and respond to infectious disease threats, wherever they occur in the world” [28]. Note that in this definition, health security describes the status of public health systems—i.e., resilience to specific threats. Given the United States’ leadership in health security agenda setting, the CDC’s conceptualisation of health security shapes and influences how public health emergencies are conceptualised (under health security framing) and addressed globally. The World Health Organisation’s (WHO) definition, although more dynamic, presents health security as “…activities required, both proactive and reactive, to minimise the danger and impact of acute public health events that endanger people’s health across geographical regions and international boundaries” [29]. However, WHO’s definition is still threat-focused—what is being secured against are acute public health events. This securitised language is echoed in the commitments made under the International Health Regulations 2005 IHR (2005) [30]. Countries are encouraged to develop the capacity to “detect, assess, report, and respond to potential public health emergencies of international concern” [31]. While such definitions have elements of “protectionism” that create a cloak of benevolence, it is important to understand who and what is being protected and the motivations behind how certain tools can be deployed to different ends.
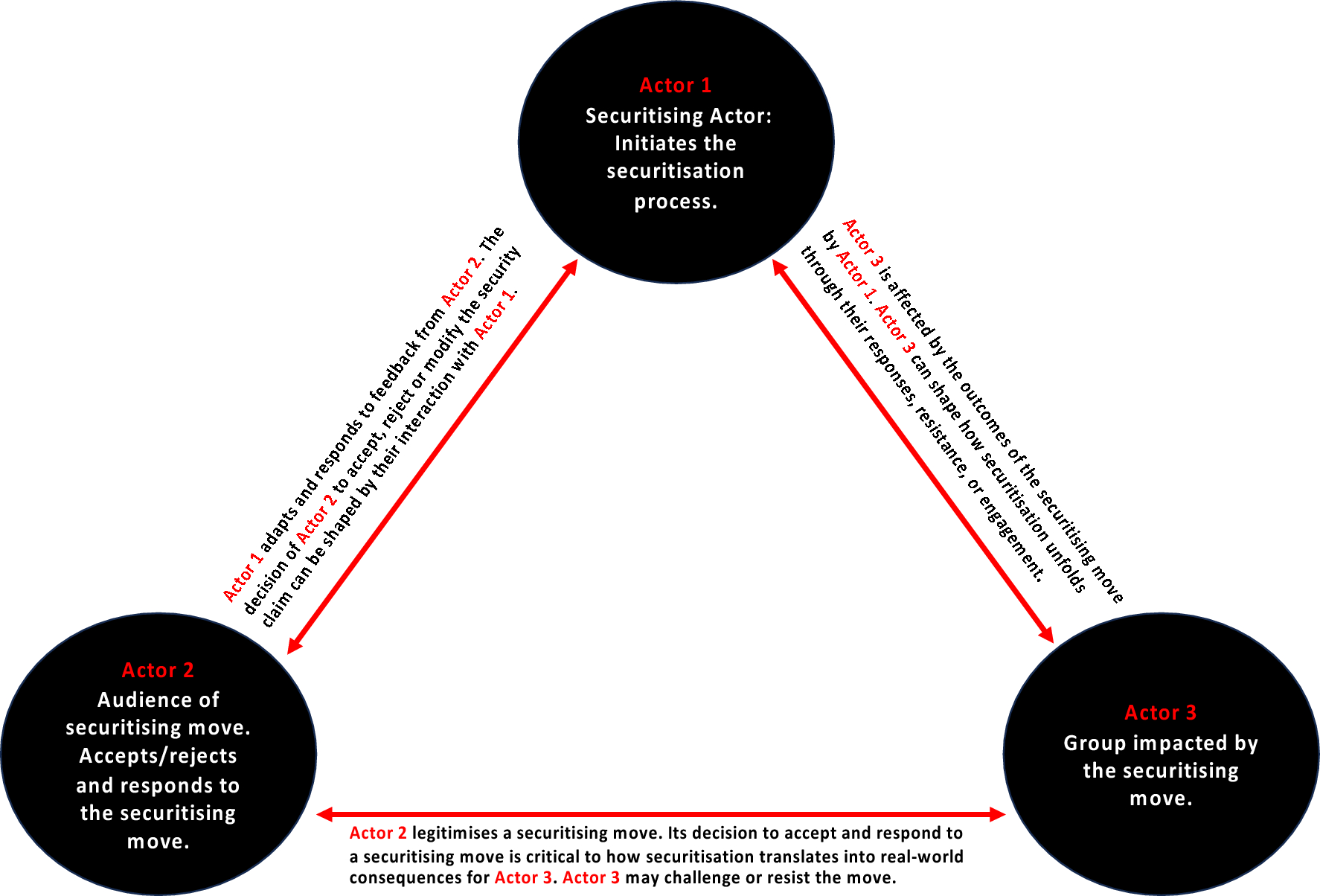
Nonetheless, there continues to be a shift towards framing health issues through a security lens [18]. It has been argued that this is because of high-income countries acting in their own self-interest [7, 34], which is seen in response to infectious disease outbreaks such as Ebola [18], Zika [19] and most recently, COVID-19 [20] because what constitutes a health security threat and who wields power to label it as such remains contentious [21,22,23]—just as in the nineteenth century, International Sanitary Conferences were contentious in terms of which (European) countries had the power to decide the fate of others [24]. At its core, the language of security creates a sense of urgency and exceptionalism [8]; however, what constitutes a threat against an individual, group, or nation is less dependent on whether the security threat actually exists but on the type of health issue and whether the political/securitising actors can successfully and effectively frame the health issue as a ‘threat’ to a potentially susceptible or welcoming audience—’’It is a choice to phrase things in security… terms, not an objective feature of the issue’’ [8, 25]. When successful and effective, a securitising move is made such that it results in mobilising multilateral/multisectoral responses and resources outside the domain of everyday politics—or “normal politics”—with the (implicit) goal of safeguarding the interests of powerful individuals, groups or nations [9, 26].
The 2014 Ebola outbreak in West Africa, which occurred during the development of the Global Health Security Agenda (GHSA), has also provided fertile ground for heightened global interest in the use of health security language and framing in the last decade—once Ebola’s potential for spread beyond its original ‘tri-border’ region was recognised internationally [34]. The everyday citizens of Guinea, Liberia, and Sierra Leone (actor 3) were not only the primary victims of the outbreak but also very much at the receiving end of securitised public health efforts in the form of coercion and containment [18] that primarily aligned itself with national security forces at the hand of its governments (actor 2)—endorsed and promoted, in part by governments of certain high-income countries and global organisations (actor 1), aligning with their own agendas and priorities. The United States (US) and the United Kingdom (UK), which were actively involved in the response, in many ways, have been at the forefront of championing practices that stem from framing health issues as security threats. This commitment is also evident in actions such as the creation of the Bureau of Global Health Security and Diplomacy by the US State Department in 2023—the latest move in its health security development timelineFootnote 3 [27]. The UK’s transformation of Public Health England into the UK Health Security Agency during the COVID-19 pandemic also nudges towards a shift and normalisation of health security framing. While such developments gather pace, there has been limited critique globally in the public health policy and practice beyond what health security means and does theoretically [4] compared to its practical impact on public health systems in different contexts, specifically in relation to individuals, groups or nations (actor 3).
The covert securitisation of health events through the declaration of Public Health Emergencies of International Concerns (PHEICs)—framing pandemics in terms of security, triggering extraordinary measures such as travel restrictions, quarantine, and large-scale mobilisation of resources—has been a driving force behind increased investment in pandemic preparedness and response activities [32, 35]. Indeed, such investments are needed. However, it is equally essential to recognise the nuanced motivations underlying such financial mobilisation. At the international level, this framing has been aligned with a tendency to prioritise national agendas over comprehensive global public health responses. This is especially the case when outbreaks extend beyond the border of their origin, most notably the 2014 West African Ebola outbreak [6, 23, 26, 32, 36], influencing how future ‘threats’ are perceived and managed. Since securitisation, an inherently undemocratic process, is often triggered in the immediate environment of a health emergency, its context-specific, longer-term impacts, especially on actor 3, are not readily considered. The urgency and exceptionalism inherent in the health security language and framing can reduce policies and practices to mere biomedical solutions rather than a deeper understanding of the political, economic and social factors intrinsic to strengthening health systems.
The perception and reality that the language and framing of health security prioritise preventing threats to Western countries, while the rest of the world is often viewed as the source of threat [37, 38], is deeply rooted in the legacy of colonisation and is well recognised [36, 39,40,41]. These patterns have persisted into the present, where former colonial powers can, through the influence of soft power, influence global narratives and priorities reinforced by their economic dominance [1, 3]. One manifestation of the awareness of such logic can be seen in Indonesia’s response to the 2006 H5N1 pandemic. Indonesia refused to share its national virus samples with the international community due to concerns about a lack of assurance of the mutual benefits of sharing samples and data, such as vaccine access [42, 43]. This refusal to share viral samples exacerbated political tensions and undermined the perceived benefits of health security—international cooperation. Such a response by Indonesia indicates the acknowledgment of the inequalities within global health governance and resistance to the inherent power imbalances within such structures [42], which manifest in different securitising moves. Sample and data sharing can no longer be viewed as merely scientific and technical in a space that has historically bred power imbalances and “uneven geographic distribution of biomedicine” [42].
Narratives such as these have continued to persist. Most recently, South Africa demonstrated high detection and surveillance capacity by sharing a new SARS-CoV-2 Omicron Strain in November 2021 [43]. However, governments of Western countries (actor 1) responded with a somewhat colonial logic directed at their population (actor 2) with dire consequences for Southern Africans (actor 3). Despite the absence of scientific evidence of the risk posed by the detection, South Africa and nearby countries were met with travel bans [44]. By this time, it was scientifically clear that detection no longer meant origin, and by the time a strain was detected, it had likely spread outside of its immediate origin [44, 45]. Nevertheless, South Africa was penalised despite demonstrating the exact capacities and capabilities advocated by the IHR for health security [32]. Scholars such as Silva and Smith have since advocated a more conditionally reciprocal approach to data sharing and collaboration during emergencies (health security events) that extends beyond symbolic expressions of solidarity – one with guaranteed equitable benefits for all countries regardless of their geographic location or economic status [43].
Ultimately, what matters is considering who is most affected by health security framing (actor 3). There is a need, for example, to consider the divide between the intended global strategies [46] and how such language and framing can unravel as action in different contexts—especially for less powerful individuals, groups, and nations (actor 3). The imperial echo of “front liners fighting” the outbreak with “targeted” responses in many ways shaped how some countries responded to COVID-19, heightening insecurities within communities by allowing the mobilisation of ‘exceptional’ governmental powers [47]. In Uganda, President Museveni’s perceived success in maintaining low COVID-19 case numbers, despite the local impacts due to the enforcement of military action and centralised authority, earned him recognition for extraordinary leadership by the British Medical Journal [48, 49]. Similarly, in the Philippines, President Duterte’s “war on drugs” was extended as a “war against COVID-19” [50], with repressive measures coming at a painful cost to communities with coercive measures [51]. Australia, often seen as more democratic, placed 3000 residents, a significant proportion from non-European backgrounds, in inner-Melbourne public housing towers under home detention [52], where members of the community found themselves without food, medicine and everyday essentials. The framing of health as a security issue supported this selective over-policing of certain communities, showcasing how securitised responses can lead to different outcomes for different groups, even within one country. What remains common across these examples is the group most impacted (actor 3)—already marginalised populations.





Comments (0)