
Remember me


Of the 449 patients who completed treatment (with nintedanib or placebo) in the INBUILD trial, 434 (96.7%) were treated in INBUILD-ON. There were 212 patients in the continued nintedanib group and 222 patients in the initiated nintedanib group. Baseline characteristics at entry into INBUILD-ON are summarised in Table 1. Mean (SD) age was 65.9 (9.9) years and mean (SD) FVC was 64.4 (17.4) % predicted; 239 (55.1%) and 79 (18.2%) patients received corticosteroids and non-biological disease-modifying anti-rheumatic drugs (DMARDs), respectively. The most commonly received non-biological DMARDs were hydroxychloroquine (3.9% of patients) and leflunomide (3.5% of patients).
Table 1 Baseline characteristics of patients at inclusion in INBUILD-ONPatient Disposition and ExposureAmongst patients who continued nintedanib in INBUILD-ON, the median (minimum, maximum) prior exposure to nintedanib in the INBUILD trial was 19.2 (12.9, 27.7) months. Amongst patients who initiated nintedanib in INBUILD-ON, the median (minimum, maximum) prior exposure to placebo in the INBUILD trial was 18.8 (13.9, 26.6) months. Median (minimum, maximum) exposure to nintedanib in INBUILD-ON was 22.0 (0.4, 38.3) months [22.1 (0.4, 38.3) months in the continued nintedanib group, 22.0 (0.4, 38.1) months in the initiated nintedanib group].
Overall, 261 patients (60.1%) completed nintedanib treatment up to week 96 (135 [63.7%] and 126 [56.8%] patients in the continued nintedanib and initiated nintedanib groups, respectively). A 96-week period of observation was completed by 266 patients (61.3%) (136 [64.2%] and 130 [58.6%] patients in the continued nintedanib and initiated nintedanib groups, respectively).
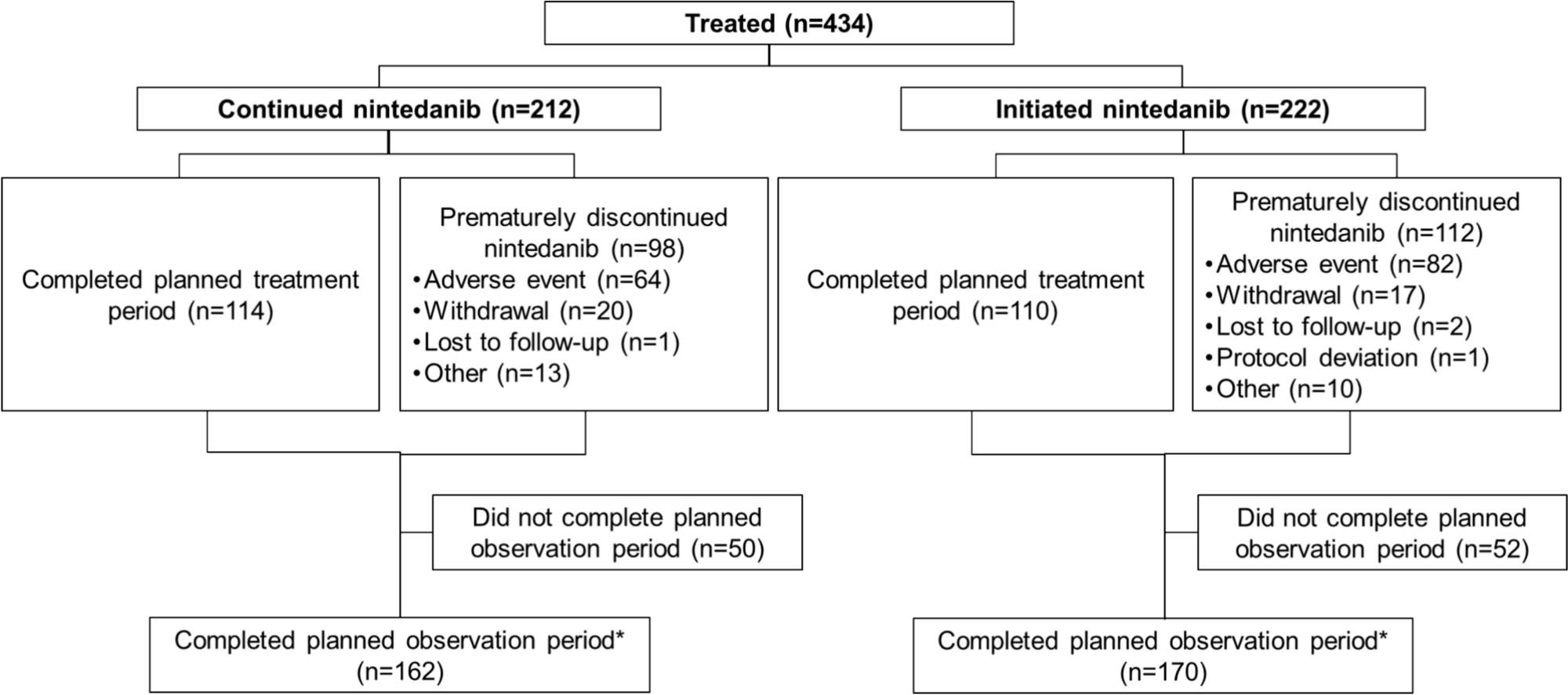
Overall, nintedanib was discontinued before the end of the planned treatment period in 210 patients (48.4%) (98 [46.2%] in the continued nintedanib group and 112 [50.5%] in the initiated nintedanib group) (Fig. 1). There was no discernible pattern in the time to nintedanib discontinuation (Figure S1). The planned observation period was completed in 332 patients (76.5%) (162 [76.4%] in the continued nintedanib group and 170 [76.6%] in the initiated nintedanib group) (Fig. 1).
Fig. 1
Disposition of patients in INBUILD-ON. *Patients who completed the last planned visit, including patients who prematurely discontinued nintedanib but completed the last planned visit, were counted as having completed the planned observation period. The protocol defined that patients should remain in the study for at least 96 weeks. Patients who could be treated with nintedanib outside of INBUILD-ON had an end-of-treatment visit at week 96. These patients were considered to have completed the planned treatment period
Adverse Events and Dose AdjustmentsDiarrhoea was the most frequent adverse event, reported at a rate of 62.0 per 100 patient-years (Table 2, Table S1). Amongst the patients who had diarrhoea, most (90.0%) experienced events of mild or moderate severity (Common Terminology Criteria for Adverse Events grade 1 or 2). Diarrhoea led to discontinuation of nintedanib at a rate of 2.7 per 100 patient-years. About 8% of patients who had diarrhoea discontinued nintedanib due to diarrhoea. Overall adverse events led to discontinuation of nintedanib at a rate of 16.7 per 100 patient-years. The adverse events that most frequently led to discontinuation of nintedanib are shown in Table S2.
Table 2 Most frequent adverse events in INBUILD-ONElevations in alanine aminotransferase (ALT) and/or aspartate aminotransferase (AST) ≥ 3 times upper limit of normal (ULN) were reported in 38 patients (8.8%) (Table S3). One patient (0.2%) had elevations in ALT and/or AST ≥ 3 times ULN and bilirubin ≥ 2 times ULN. Major adverse cardiovascular events were reported at a rate of 4.1 per 100 patient-years (Table S4). Bleeding adverse events were reported at a rate of 7.1 per 100 patient-years (Table S5). The most frequently reported bleeding adverse event was epistaxis, which was reported at a rate of 1.5 per 100 patient-years.
Serious adverse events were reported in 234 patients (53.9%), at a rate of 37.2 per 100 patient-years. A total of 190 patients (43.8%) had serious adverse events that required or prolonged hospitalisation. The most frequent serious adverse event was pneumonia, which was reported in 36 patients (8.3%) and at a rate of 4.5 per 100 patient-years (Table 3). Fatal adverse events were reported in 77 (17.7%) patients, at a rate of 9.5 per 100 patient-years. Progression of ILD was the most frequent fatal adverse event (rate of 1.2 per 100 patient-years).
Table 3 Most frequent serious adverse events in INBUILD-ONOverall, 359 patients (82.7%) received nintedanib 150-mg bid as their first dose in INBUILD-ON (143 [67.5%] patients in the continued nintedanib group and 216 [97.3%] patients in the initiated nintedanib group). In total, 147 patients (33.9%) had ≥ 1 dose reduction (42 [19.8%] and 105 [47.3%] patients in the continued nintedanib and initiated nintedanib groups, respectively) and 175 patients (40.3%) had ≥ 1 treatment interruption (79 [37.3%] and 96 [43.2%] patients in the continued nintedanib and initiated nintedanib groups, respectively). The median (minimum, maximum) total duration of treatment interruptions was 25 (1, 197) days in the overall trial population (22 [1, 197] days in the continued nintedanib group and 27 [1, 176] days in the initiated nintedanib group).
Changes in FVCIn total, 222 (51.2%) patients had missing FVC data at week 48, of whom 79 patients had discontinued nintedanib. At week 96, 204 (47.0%) patients had missing FVC data, of whom 158 patients had discontinued nintedanib. Based on the observed data, there was a gradual decline in FVC during INBUILD-ON (Fig. 2). Mean (SE) change in FVC from baseline to week 48 of INBUILD-ON was − 71.6 (16.1) mL [− 128.5 (25.5) mL in the continued nintedanib group and − 14.8 (18.2) mL in the initiated nintedanib group]. As a comparator, the mean (SE) change from baseline to week 52 in the nintedanib group of the INBUILD trial was − 75.1 (15.4) mL (Figure S2).
Fig. 2
Change from baseline of INBUILD-ON in FVC (mL) in a all patients and b patients who continued nintedanib or initiated nintedanib in INBUILD-ON
Mean (SE) change in FVC from baseline to week 96 of INBUILD-ON was − 130.9 (16.4) mL [− 135.3 (17.6) mL in the continued nintedanib group and − 126.2 (28.5) mL in the initiated nintedanib group]. Absolute declines in FVC % predicted > 5% and > 10% from baseline to week 96 of INBUILD-ON were observed in 45.0 and 19.1% of patients (Figure S3). Absolute declines in FVC % predicted > 5% from baseline to week 96 of INBUILD-ON were observed in 48.5 and 41.7% of patients in the continued and initiated nintedanib groups, respectively. Absolute declines in FVC % predicted > 10% from baseline to week 96 of INBUILD-ON were observed in 17.7 and 20.4% of patients in the continued and initiated nintedanib groups, respectively.
Time-to-Event EndpointsOverall, 83 patients (19.1%) died; 190 patients (43.8%) had ILD progression (absolute decline in FVC % predicted > 10%) or died; and 99 patients (22.8%) had an acute exacerbation or died.
Comments (0)